
Download the webinar slides here
Learning objectives of the webinar
Our goal is to empower individuals living with pulmonary hypertension and their families, equipping them with actionable insights and practical knowledge.
- What the new guidelines on pulmonary hypertension say about pregnancy
- What is new with respect to the previous guidelines
- Understanding the physiology and why pregnancy is challenging in pulmonary hypertension
- Pulmonary hypertension and contraception
- How to manage pregnancy in pulmonary hypertension
- Future outlook
Transcript
“BALANCING LIFE AND HEALTH: PULMONARY HYPERTENSION, WOMEN AND FAMILY PLANNING”, September 5, 2023
NB. This transcript can be translated into your preferred language – use orange button at the bottom centre of this page to select it. The slides are not translatable.
DISCLAIMER: Despite every effort to ensure the accuracy of this transcript, we strongly encourage all visitors to consult with their healthcare professionals before making any decisions based on the information provided. Additionally, while the quality of Google Translate has improved tremendously in recent years, please remember that it is an automated service and not a human translation.
DR. ANDREAS REIMANN
Welcome to the third of our webinar series on the latest pulmonary hypertension guidelines from the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). My name is Andreas Reimann, representing admedicum, and we’re proud to support the Alliance for Pulmonary Hypertension, a non-profit organization based in Brussels dedicated to facilitating knowledge exchange on pulmonary hypertension. This webinar, like its predecessors, will also be accessible as a recording on the pulmonary hypertension knowledge sharing platform.
Previously, we explored topics such as patient-reported outcome measures and the importance of shared decision-making between patients and healthcare providers. Today, we delve into a more intimate theme: family planning and pregnancy. It’s my privilege to introduce three distinguished speakers who will offer their insights from varied perspectives. Pisana Ferrari, Secretary General of the Alliance for Pulmonary Hypertension, will share her experiences and patient-centric views. Professor Dr. Karen Olsson from the Medical School of Hannover and Dr. Esther Nossent from the University of Amsterdam Medical School, both renowned pulmonologists, will discuss clinical aspects of the subject. We are grateful to have Pisana begin the discussion with her personal journey and professional insights.
PISANA FERRARI
Good afternoon and good morning to those joining from different time zones. I’m deeply honored to have been invited to speak on a topic of significant importance within the field of pulmonary hypertension. For those who may not be familiar with me, I was a pulmonary hypertension patient for 14 years and I underwent a double lung transplant 21 years ago. Since then, I’ve dedicated myself to patient advocacy, serving currently as the President of the Italian Patient Association and Secretary General of the Alliance.
Today, I’ll begin my presentation with patient testimonies that I’ve gathered from discussions on message boards and through pulmonary hypertension International. These testimonies, which I will quote in the following slides, offer profound insights into the experiences and challenges faced by those living with pulmonary hypertension, particularly in the context of family planning and pregnancy.
- “Not all patients are interested in having children, but for some, it’s a continuous trauma to overcome, especially in the fertile age and the society we find ourselves in.”
- “I always told myself, well, we can adopt. But I was advised not to because children carry diseases.”
- “It’s like having a wound that’s always open, even though over time you learn to live with it.”
- “The topic of children is very delicate. I have been living with choices made and choices forced upon me for 20 years. The weight on the conscience is heavy.” [patient who had an abortion]
- “There’s certainly no right way to say it, and the abrupt way is probably more impactful, but one should think about the sensitivity of the other person, and recommend psychological support.”
- “I was on a waiting list for a transplant and could not get a health certificate for the judge, so it was not possible to adopt. We decided for surrogacy. This is a criminal offense in my country, we had to go abroad.”
- It’s been two years, but I am still going around shops for children’s clothes and imagining myself with a baby in my arms”
- “I initially found out about it online, then the PH center called me while I was driving, saying they had forgotten to tell me. Closed doors and those words that still resonate.”
- “At my PH center, they described pregnancy as flipping a coin. One doctor said that the very mention of the word made his hair rise on the back of his head.”
- “I was prevented from having ovarian stimulation [for in vitro fertilization] as PH could worsen.“
- “The constant anxiety about contraception adds to an already restricted sex life. More efforts should be made to help in this aspect as well.”
- “The issue with pregnancy influenced my relationship with my ex-partner; it was hard for him to accept it and also for his family.”
- “If they tell you that for a pregnancy you should suspend all medications and spend 9 months in hospital, who would do that? Currently, I believe there are no medications compatible with pregnancy.”
- ‘I always thought that a child should not be allowed to have the same thing that happened to me, and my mother” [male patient with familial PH who lost his mother to PH as a child]
- “I always dreamed to be a mother. This dream has been crushed.”
The testimonies illustrate a spectrum of emotions and decisions, from the struggle with the desire for children amidst societal pressures, to the heart-wrenching decisions around abortion, adoption, and surrogacy. One poignant testimony reveals the deep emotional impact of being advised against adoption due to health risks, while another shares the journey to surrogacy, a path fraught with legal and emotional challenges. These stories not only shed light on the personal struggles but also highlight the societal and familial pressures women face.
From a healthcare perspective, these testimonies underscore the complex interplay between patient desires, medical advisories, and the harsh realities imposed by pulmonary hypertension. They reveal a pressing need for empathetic communication, accurate information, and support for individuals navigating these deeply personal decisions. The absence of a scientific consensus on family planning within the context of pulmonary hypertension further complicates the issue for both patients and healthcare providers.
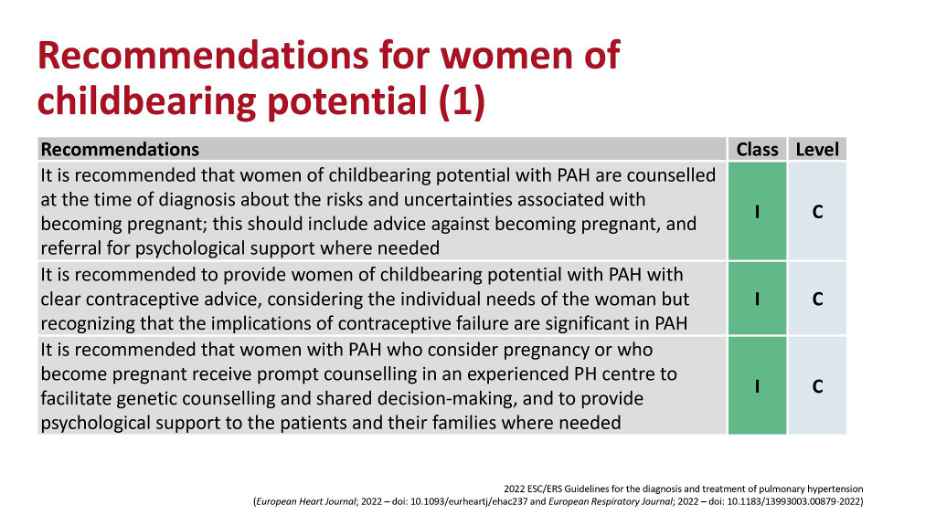
Today’s discussion also focuses on the new guidelines from the European Society of Cardiology, which adopt a more nuanced approach to pregnancy and pulmonary hypertension. Unlike the 2015 guidelines, the latest recommendations emphasize the importance of counseling women about the risks and uncertainties, advising against pregnancy while ensuring support is available for those in need. This represents a significant shift towards acknowledging the complexity of these issues and the necessity of informed, shared decision-making.
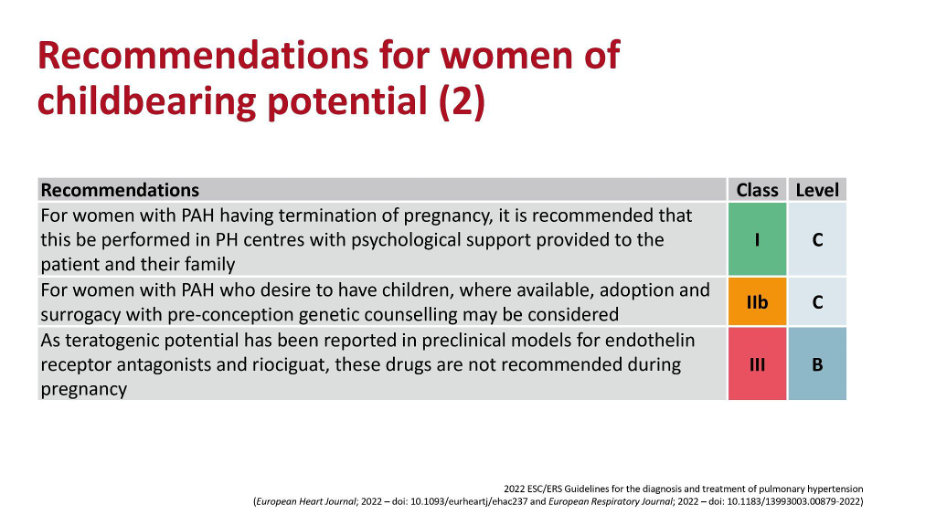
As a member of the task force that contributed to the new guidelines, I had the privilege of infusing the patient perspective into our deliberations. This has resulted in a more comprehensive and participatory approach, acknowledging the diverse needs, beliefs, and circumstances of individuals affected by pulmonary hypertension. The guidelines now consider adoption, surrogacy, and genetic counseling as part of the conversation, marking a pivotal step forward in addressing this sensitive issue.
To conclude, while the conversation around pregnancy and pulmonary hypertension remains challenging, the evolving landscape of medical research and guidelines offers hope. The journey towards understanding and managing pulmonary hypertension continues, with each advancement bringing us closer to better outcomes and quality of life for patients. My journey from diagnosis to advocacy reflects this evolution and underscores the importance of hope and patient-centered care. I was diagnosed with pulmonary hypertension when I was in the late stage of my pregnancy. It was a very difficult journey, but today things are very different and in future they could be even better and I would like to end with that note of hope. Thank you very much for your kind attention.
DR. ANDREAS REIMANN
Thank you, Pisana, for sharing both your personal journey and the powerful testimonies of patients. This deeply personal and touching subject highlights the evolving nature of the medical field concerning pulmonary hypertension .
We are grateful for these insights. Now, we look forward to hearing from Dr. Karen Olsson, who will share the latest news and findings on pregnancy and pulmonary hypertension.
DR. KAREN OLSSEN
Thank you for the introduction. I’ll briefly share my screen to discuss a topic that has become more than just a project to me—pulmonary hypertension and pregnancy. It’s evolved into a lifelong task. The stringent recommendations around pregnancy in pulmonary hypertension stem from historical guidelines and data, which I’ll overview to shed light on the reluctance around pregnancy in pulmonary hypertension patients.

In 2009, guidelines starkly recommended avoiding pregnancy in pulmonary hypertension patients, a stance unchanged by 2015. However, the reality diverged as patients still became pregnant, necessitating emergency therapies. This contrast between guidelines and patient experiences underscores the challenge in managing pulmonary hypertension during pregnancy.
Pregnancy poses significant risks due to physiological changes, such as increased blood volume and cardiac output, alongside decreased systemic resistance. These changes can precipitate right heart failure in pulmonary hypertension patients.
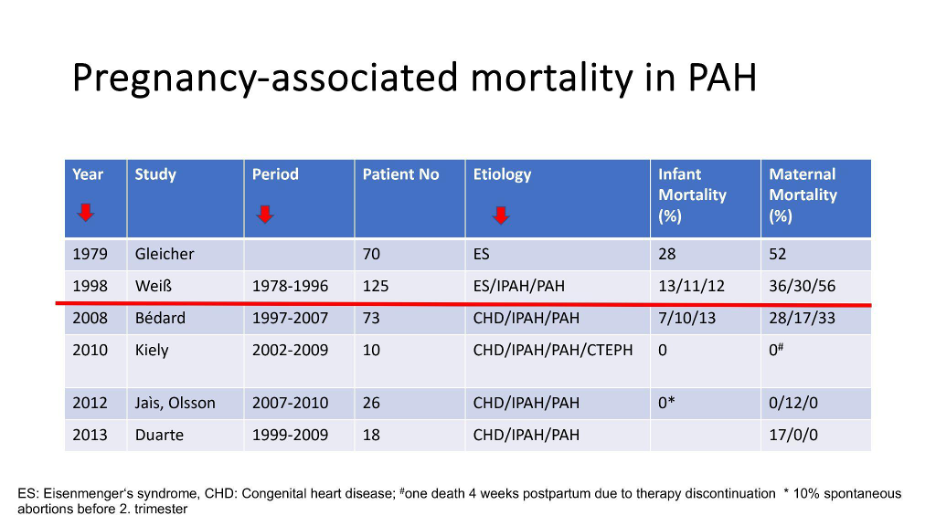
Data from developed countries shows a declining maternal mortality rate in pulmonary hypertension patients over the years, thanks to advancements in therapy. Earlier studies reported mortality rates as high as 56%, but more recent studies show a significant reduction, with some reporting no maternal deaths. This improvement is attributed to better management and therapies for pulmonary hypertension.
Patients on calcium channel blockers or those with controlled pulmonary hypertension on therapy are at lower risk during pregnancy. In contrast, those with uncontrolled pulmonary hypertension or high pulmonary vascular resistance face higher risks, especially under general anesthesia or in emergency settings.
At Hannover Medical School, we’ve developed an algorithm for managing pregnant pulmonary hypertension patients, emphasizing rapid consultation, clinical assessment, and a multidisciplinary approach, including shared decision-making:
- We monitor patients closely; every 6-12 weeks during first trimester, every 2-4 weeks during second and thirds trimester focus on echocardiography,
- We test NT-proBNP and fetal development
- Plan deliveries around the 38th gestational week, avoiding general anesthesia to minimize risks.
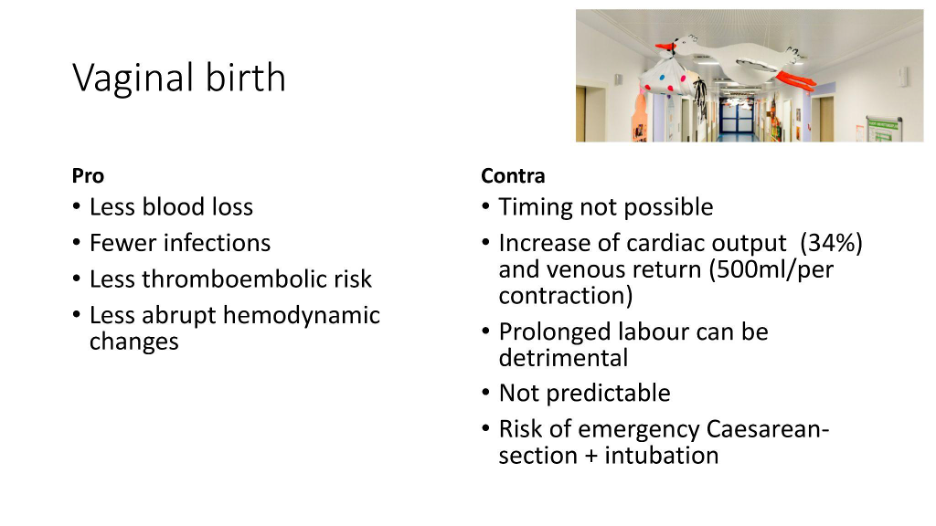
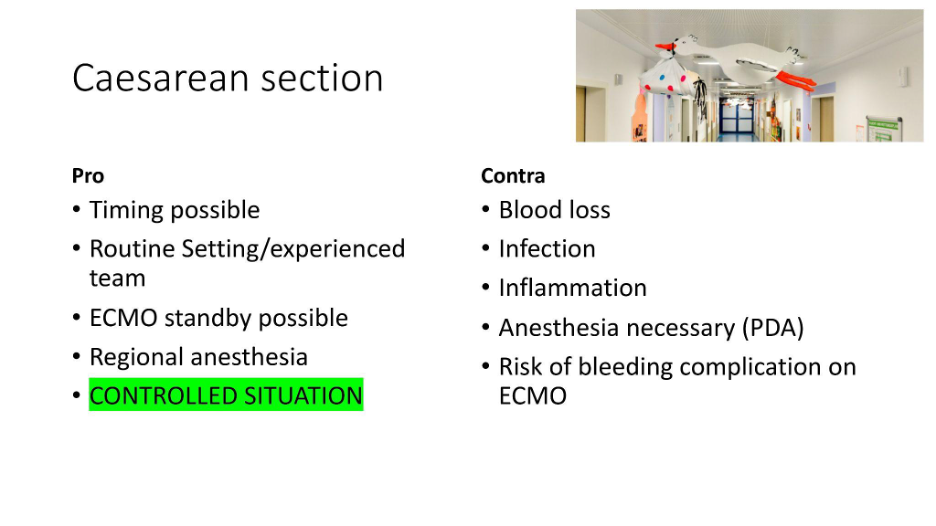
The mode of delivery is a critical decision. Vaginal birth offers some benefits, like less blood loss and thromboembolic risk, but unpredictability and potential for emergency situations make cesarean section often preferable for its controlled environment and experienced team .
The management of pregnancy in patients diagnosed with pulmonary arterial hypertension presents a complex challenge, requiring meticulous control within standardized clinical settings. Among the primary concerns in such patients is the administration of Prostaglandin E, which, while essential, introduces risks including significant blood loss, infection, inflammation, and the necessity for anaesthesia. Moreover, the potential requirement for additional ovocyte retrieval amplifies the risk of hemorrhagic complications.
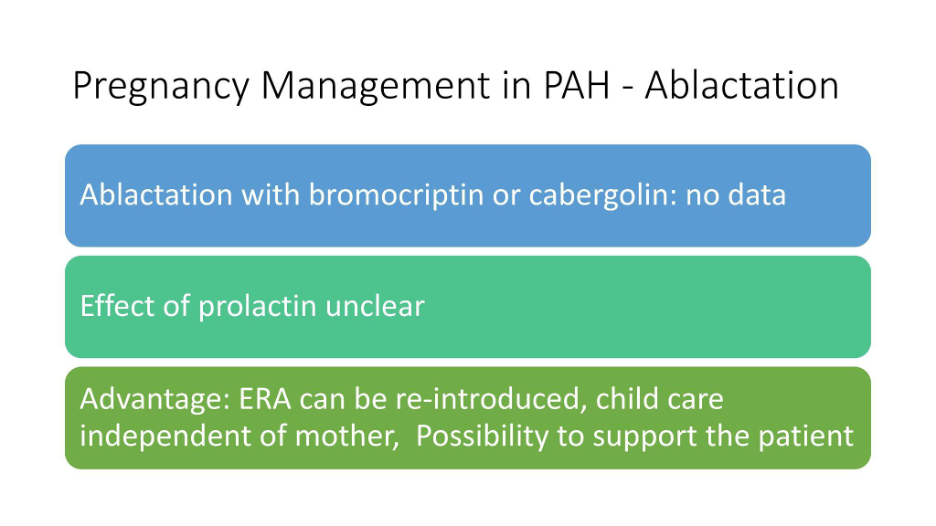
There is so much debate about the practice of ablactation. Currently, there is a lack of data regarding its implementation and benefits, particularly in the context of postpartum cardiomyopathy and the potentially adverse effects of prolactin levels. Nevertheless, ablactation offers the advantage of allowing therapy reintroduction, ensuring childcare is not solely dependent on the mother, thus facilitating her recovery.
Despite ongoing research, several questions remain unanswered, especially regarding the pregnancy risk in patients with controlled pulmonary arterial hypertension, the impact of pregnancy on disease progression, and the optimal management strategies for severe pulmonary arterial hypertension cases during pregnancy. Our paper aims to address these queries, reporting on outcomes that, while moderately favorable, also include instances of adversity.
Our study encompassed 525 pregnancies in 16 women from 2007 to 2017, with a notable success rate and one case of a German’s pregnancy leading to a positive outcome. We observed normal development in offspring, with 14 out of 16 patients maintaining stable conditions post-delivery; however, two required lung transplants, and a third patient also underwent transplantation subsequently. The rate of spontaneous abortions aligned with general expectations, yet we documented a concerning trend of condition worsening in six patients 9 to 22 months postpartum, albeit stabilization was achieved with intensified medical treatment.
In conclusion, pregnancy in patients with pulmonary arterial hypertension remains fraught with risks and uncertainties, despite improved outcomes in the era of modern treatment. It underscores the necessity for a nuanced, individualized approach, incorporating current data and uncertainties into the decision-making process. Emphasizing expert consultation, shared decision-making, and standardized care will ensure the highest quality of management for our pulmonary arterial hypertension patients during pregnancy.
Thank you very much .
DR. ANDREAS REIMANN
Thank you very much, Karen, for the enlightening presentation and for sharing your in-depth knowledge with us. It is worth noting at this point that Karen is not only sharing her expertise but is also a co-author of the upcoming guidelines as Pisana. This provides us with firsthand experience and insights, which is Valuable.
I am now honoured to introduce Esther Nossent from Amsterdam. Esther is a distinguished pulmonologist who not only excels in her medical practice but also leads and collaborates with multidisciplinary teams. Her work notably extends to vital discussions on birth control and family planning, addressing the comprehensive needs of her patients.
Esther, the floor is yours to share your expertise and perspectives on these crucial issues.
DR. ESTHER NOSSENT
Thank you for your introduction, and I appreciate the opportunity to share my thoughts today. I aim to discuss the complex issue of managing pulmonary hypertension in relation to family planning, birth control, and pregnancy, as emphasized by recent guidelines. Our focus is on the critical aspects of birth control options for those living with pulmonary hypertension, a topic that has been previously touched upon by other speakers.
A few weeks ago, I was prompted to speak on this subject, which reminded me of a patient who recently collapsed at a party and was diagnosed with idiopathic pulmonary arterial hypertension. Her case underscores the essence of our discussion today: the intersection of pulmonary hypertension management and the desire to start a family, a deeply personal and varied decision for each patient.
In managing pulmonary hypertension, it’s paramount to adopt a multidisciplinary approach, especially in primary hypertension centers, to address the myriad of considerations surrounding family planning. This approach aligns with the latest guidelines and necessitates a comprehensive model of care that not only focuses on the patients but also involves their partners and families from the diagnosis stage.
Key considerations include the impact of pulmonary hypertension medications on pregnancy, the risks associated with pregnancy in pulmonary hypertension patients (such as maternal and fetal mortality, worsening of the disease, and potential for heart failure), and the nuanced decision-making process regarding pregnancy. It’s imperative to navigate these discussions with individualized advice, taking into account the patient’s specific condition, medication regimen, and the severity of their pulmonary hypertension.
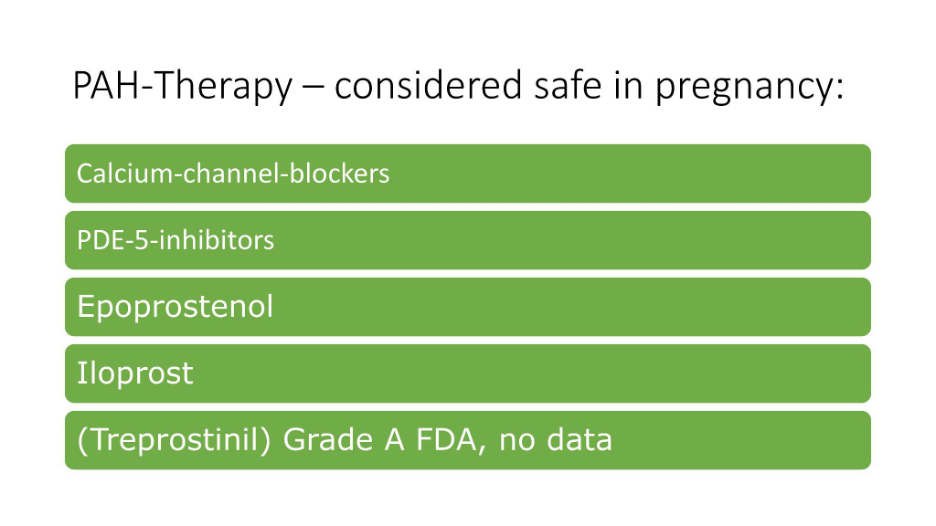
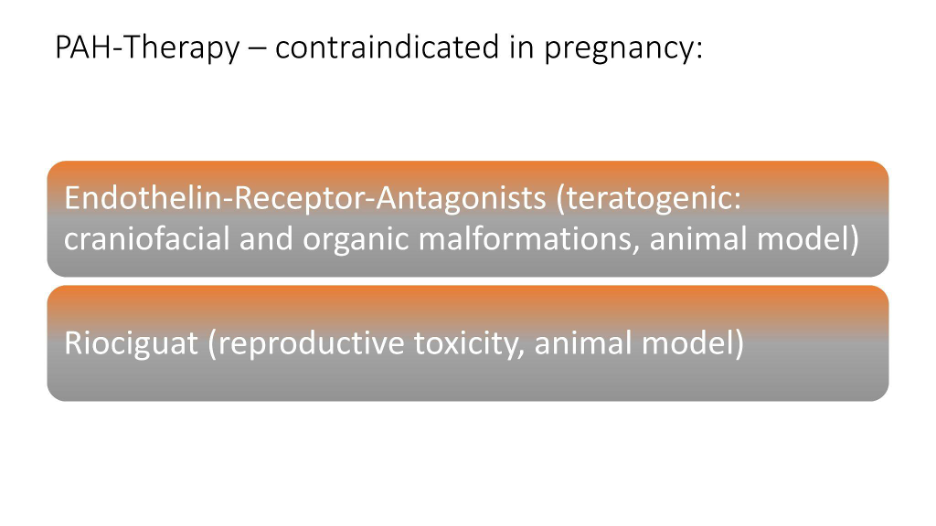
Regarding the treatment of pulmonary hypertension and its implications for pregnancy, we focus on medications targeting three main pathways, notably the endothelin pathway, which includes drugs like bosentan, macitentan, and ambrisentan. Specifically, macitentan poses risks to the fetus and should be discontinued during pregnancy, akin to the necessary precautions with other select medications. While data on the safety of sildenafil, tadalafil, and epoprostenol during pregnancy are limited, these medications are generally considered safe and can be used.
A recurring query, especially in recent months, concerns sotatercept, an emerging medication for pulmonary hypertension. Anticipated to be approved in various European countries soon, sotatercept shows promise for significantly improving the management of pulmonary arterial hypertension, potentially enhancing pregnancy outcomes for patients. However, its safety during pregnancy remains undetermined due to the absence of data, particularly because its large molecular size may prevent it from crossing the placenta. This aspect remains a critical area for further research.
In discussions with patients about birth control, pregnancy, and family planning, it is crucial to navigate these topics with detailed information and personalized guidance. This approach ensures that patients are well-informed about their medication options and the associated risks and benefits, facilitating informed decision-making in line with the latest guidelines and individual health considerations.
Furthermore, the conversation extends to birth control methods, where considerations must be made for the potential risks and effectiveness of various contraceptives in the context of pulmonary hypertension. The importance of a team-based approach is highlighted, involving specialists from gynecology, pediatrics, anesthesiology, and more, ensuring a holistic and informed decision-making process.
Family planning: issues to consider
Preconception genetic counseling and the possibility of preimplantation genetic testing in some countries ( not available in every country as it needs Invitro fertilization which is risky ).
It’s important to ensure not to give the disease to your offspring specially if you have an inheritable form of pulmonary hypertension. a very sensitive thing.
Birth control
Barrier Contraceptive Methods: Condoms are safe for patients with pulmonary hypertension though their reliability can vary.
Oral contraceptives: Hormonal contraceptives containing estrogen increase the risk of thromboembolism (blood clots in legs or lungs), which can exacerbate pulmonary hypertension. The use of bosentan reduces the effectiveness of most hormonal contraceptives, making them less reliable.
Intrauterine Devices: Generally safe for patients, but insertion may cause vasovagal reactions, poorly tolerated by some pulmonary hypertension patients. Copper intrauterine devices may increase the risk of infection, a concern particularly for patients with congenital heart disease.
Sterilization
Female sterilization, including hysteroscopic sterilization which is preferred and tubal ligation involves surgical procedures with risks, including the risk of general anesthesia.
Male sterilization (vasectomy) is less risky, can be done under local anesthesia, and generally has fewer complications.
This discussion highlights the importance of tailored family planning, birth control, and pregnancy guidance for patients with pulmonary hypertension. It’s a delicate subject that requires open dialogue and informed decision-making, aiming for the best possible outcomes for each patient. Let’s continue this important conversation.
Andreas Reimann
Thank you, Esther, for sharing your insights on birth control and family planning in the context of pulmonary hypertension. To summarize, it seems that the presentation leaned towards recognizing opportunities while also advising caution. Please feel free to correct me if my interpretation is off, and we can clarify further shortly.
We’ve received an initial comment from Melanie, highlighting the delicate timing required to inform female patients about pregnancy considerations. Melanie points out the importance of early discussion to ensure patients fully understand the implications without feeling overwhelmed or discouraged from pursuing treatment. This is a crucial balance to strike, emphasizing the sensitivity required in these conversations.
This topic opens the floor for further discussion, so I encourage everyone here to share their questions or remarks using the chat function. Let’s continue this engaging dialogue.Karen, would you like to begin?
PROF. KAREN OLSSON
Melanie raises a crucial point about the timing of discussing pregnancy with female patients.
The guidelines suggest addressing pregnancy as early as feasible, ideally at the time of diagnosis.
Initially, it’s essential to clarify that pregnancy is not advisable due to potential dangers and the need for therapy evaluation.
The comprehensive discussion on pregnancy should be postponed until therapy has been established and the patient’s condition is assessed.
Later, a thorough risk evaluation should take place to revisit the topic of pregnancy with updated information and considerations.
At diagnosis, it’s critical to emphasize that pregnancy is dangerous and not an option before effective therapy is in place.
It’s important to maintain an open line of communication, revisiting the discussion on pregnancy as the patient’s condition and treatment progress.
Andreas Reimann
Any remarks from Esther ?
Dr. Esther Nossent
I concur with the sentiment but emphasize the overwhelming amount of information and considerations patients face upon diagnosis, as highlighted by patient testimonies.
These underscore the necessity of tailoring the timing and depth of discussions to each patient’s unique situation and readiness.
While I appeared more cautious compared to Karen, the core agreement is on the importance of focusing on the emerging opportunities within the updated guidelines and evolving professional and patient perspectives.
I emphasize the critical need for a detailed, personalized risk assessment to navigate the possibilities cautiously.
I also recognizes that every patient has unique desires and circumstances, which must be considered in the decision-making process.
DR. ANDREAS REIMANN
Thank you.
Pisana. I’m interested in understanding the role of patient organizations in facilitating communication between women contemplating pregnancy while living with pulmonary hypertension and those who have already navigated this journey. This includes sharing experiences of both successful and unsuccessful pregnancies. The value of these exchanges lies in the support they offer and their potential to aid in making well-informed decisions.
Pisana Ferrari
Discussing infertility is an immensely personal and sensitive subject. Many women are hesitant to openly discuss it, a reality I encountered firsthand when initiating a conversation on this topic through a message board on pulmonary hypertension international forums. Despite my expectations for more exchange, the response was not much . The pain and difficulty in speaking about such deeply personal experiences are palpable. Through these discussions, there have been stories of heartache, but also tales of hope, including successful surrogacies and adoptions. Societal pressures undeniably play a significant role in this narrative. In certain cultures, including my own in Italy, motherhood is highly esteemed, and the inability to conceive can strain relationships and intensify personal and familial distress. Regrettably, to my knowledge, there is a lack of a dedicated space where women can share and find solace in their experiences with infertility.
PROF. KAREN OLSSON
I agree with you Pisana.
Engaging with the topic of pregnancy in our patient forums, we’ve observed a diverse array of experiences across Europe, particularly among German-speaking countries, drawing individuals eager to discuss this sensitive issue. My outlook might be perceived as more optimistic, yet it’s grounded in extensive experience. Today, however, marks a challenging day to broach this subject, as we faced the heart-wrenching decision of prioritizing a mother’s life over her unborn child’s. Despite such dire situations, we often manage to save lives, including those diagnosed with potentially fatal conditions, extending their lives significantly.
Every case presents a unique discussion, underscoring the importance of individualized care. Today’s decisions, although difficult, highlight the critical role of removing judgment from our professional actions and embracing shared decision-making whenever possible. My early career frustration stemmed from an avoidance culture surrounding pregnancy discussions, which we are now striving to change.
Our goal is to standardize care, generate data, and ensure the delivery of the highest quality medicine to our patients. While we cannot guarantee pregnancy for every patient, our advocacy must focus on providing the best medical care possible, it’s fundamental .
PISANA FERRARI
Reflecting on my journey, it’s remarkable to consider that thirty-five years ago, during my pregnancy, I was diagnosed with a condition for which there were no available treatments, no specialist centers, and no clinical guidelines to follow. At that time, resources and support were virtually non-existent. Yet, looking at how far we’ve come since then fills me with hope. The medical field has seen incredible advancements, with significant progress in drugs, expert care, and comprehensive clinical guidelines. This evolution makes me optimistic about the future, believing that continued advancements will bring even greater improvements. It’s a testament to how much has changed, and it’s a reminder that we have every reason to be hopeful for what’s to come.
DR. ANDREAS REIMANN
What we observe is that making decisions about pregnancy, birth control, and family planning for patients with pulmonary hypertension is highly personal and necessitates informed guidance from specialized centers. The Alliance for Pulmonary Hypertension offers global resources through its knowledge-sharing platform, which is invaluable for accessing current information and support. For female pulmonary hypertension patients who are not in proximity to our centers, seeking out pulmonary hypertension specialists who possess a deep understanding of how the condition intersects with pregnancy and family planning is crucial. Karen, could you share your advice?
PROF. KAREN OLSSEN
I’m not certain, but answering questions about what we commonly encounter can be challenging. For instance, we often receive inquiries from patients worldwide, including Africa, about managing pregnancy. If these patients visit their local healthcare centers, they’ll find that we are well-connected and communicate effectively with one another, allowing them to be referred to centers with more expertise when necessary. However, challenges remain due to variations in resources, medications, and available options across different countries. For example, a woman in Africa might not have access to the same medications or level of medical care, or may not be able to afford certain treatments if she chooses to pursue them. Despite these challenges, communication and networking play a crucial role, and there’s a need to enhance our efforts in these areas. We aim to address these issues more comprehensively, starting with initiatives on a European level, in hopes of making a broader impact soon.
DR. ESTHER NOSSENT
I agree with Karen’s assessment. Achieving high-quality primary care worldwide is a challenging yet essential goal. Particularly in the context of this topic, we face significant tasks and unanswered questions that need to be addressed in the coming years. Moreover, it’s crucial to ensure that knowledge and quality care are accessible in every country, although this requires overcoming numerous obstacles.
DR. ANDREAS REIMANN
Yes, and the pulmonary hypertension knowledge sharing platform serves as an excellent resource for information dissemination and collaboration. We plan to make this and other valuable content available on the platform so everyone can access it anytime. I strongly encourage all webinar participants to share this content with other patient communities and, if feasible, translate it into local languages or host small webinars in your communities to further disseminate this information.
Regarding the topic of adoption discussed in the chat, it’s often required that a medical statement vouches for the mother’s future capability to care for the child. Predicting the future is inherently challenging, as no one has the ability to foresee what lies ahead. I’m interested in whether there has been a shift in perspective among young women who wish to adopt children.
Has there been any change in how this issue is approached or perceived?
PROF. KAREN OLSSEN
Answering this question is complex, as it varies based on the living conditions in different European countries. Specifically in Germany, health restrictions exist, and individuals are required to obtain certificates, as previously mentioned. These certificates must indicate that one’s life expectancy is not significantly impaired, among other proofs of well-being. This requirement can make adoption challenging or even impossible for some, even if the patient is in good health. Therefore, it’s a contentious issue. Like other sensitive topics such as organ donation and surrogacy, laws and perspectives may evolve in the coming years, though it’s uncertain when these changes will occur.
DR.ESTHER NOSSENT
Certainly, the introduction of new medications has significantly improved life expectancy compared to what it was 20 years ago. This progress has been beneficial for those affected by conditions that are now more manageable with these treatments. However, the impact and accessibility of these advancements can vary widely depending on the European country in question, as each nation has its own set of healthcare regulations and policies.
DR. ANDREAS REIMANN
Thank you, Pisana. To conclude, what message would you like to leave with all the women who have watched us today or will watch us in the future?
PISANA FERRARI
I believe that all women with pulmonary hypertension should receive treatment at an expert center. This is my main recommendation, not only for pregnancy but for all aspects of care. It’s crucial to solving the problem. Unfortunately, this isn’t yet happening, and it’s essential that it becomes so.
DR. ANDREAS REIMANN
Thank you very much, Dr. Nossent, Prof. Olssen, and Pisana Ferrari, for joining us today. I invite everyone to join us again on October 12th, when we will be discussing the updated treatment algorithm for pulmonary hypertension with the very renowned experts, Marius Hoepper and Olivier Sitbon. Stay tuned for that, and I wish you all a very pleasant rest of your day. Thank you again, and goodbye.
Warmest thanks to
- The speakers Karen M. Olsson MD, Dr. Esther J. Nossent and Pisana Ferrari
- The patient engagement experts admedicum for the organisational and technical support
- To Dr. Andreas Reimann, Managing Partner of admedicum, for moderating the discussions.