
“THE RISE OF PULMONARY HYPERTENSION ASSOCIATIONS AND HOW THEY ARE SHAPING TODAY’S CARE LANDSCAPE”, December 12, 2023
NB. This transcript can be translated into your preferred language – use orange button at the bottom centre of this page to select it (slides are not translatable).
DISCLAIMER: Despite every effort to ensure the accuracy of this transcript, we strongly encourage all visitors to consult with their healthcare professionals before making any decisions based on the information provided. Additionally, while the quality of Google Translate has improved tremendously in recent years, please remember that it is an automated service and not a human translation.
ROBERT PLETICHA, MODERATOR
Short welcome message and introduction of speakers
PISANA FERRARI
The history of pulmonary hypertension measurement and understanding extends well beyond 1967, tracing back to the late 19th century. However, the 1960s were relatively uneventful in this context until an epidemic caused by an appetite suppressant drug emerged. The first cases were reported in Switzerland, Germany, and Austria, with around 600 individuals affected by 1985.
This incident significantly reignited interest in pulmonary hypertension, leading to the first pulmonary hypertension symposium in Geneva, Switzerland. This event, sponsored by the American Heart Association and the World Health Organization, focused on primary pulmonary hypertension, now known as idiopathic pulmonary hypertension, and marked the inception of the first official pulmonary hypertension classification.

The first pulmonary hypertension symposium was a modest gathering of 17 individuals, but by the time of the last symposium in Nice, attendance had surged to over 2,000 participants, illustrating the growing interest and advancements in the field. In 1981, the National Institutes of Health in the United States established the first patient registry for pH, including 187 patients from 1981 to 1985.
Another significant milestone occurred in 1982 when Sir John Vane received the Nobel Prize for his discovery of prostacyclin, a critical advancement in pulmonary hypertension treatment.
The mid-1990s witnessed the initiation of trials for epoprostenol, a prostacyclin analogue, leading to the first randomized trials. This period also saw the public launch of the World Wide Web, which played a pivotal role in disseminating knowledge about pulmonary hypertension . By the 1990s, a wealth of information from pathology studies, the US National Institute for Health registry, and clinical trial findings was available, leading to the approval of Flolan, the first pulmonary arterial hypertension specific medication. This era marked the beginning of research and web into new potential treatments and the initiation of the first lung transplant programs, notably by the surgeon who operated on me in the late 1980s to early 1990s.
The first patient support group in the United States was established during this period, offering a vital lifeline to those diagnosed with pulmonary hypertension when no treatments or specialized centers were available. The Pulmonary Hypertension Association went online, creating a message board that significantly impacted many, including me, by reducing feelings of isolation and connecting patients with each other.
I now pass the discussion to Matt, who will share insights into his pioneering efforts within the pulmonary hypertension association movement, specifically focusing on the development and impact of the Pulmonary hypertension association.
Matt Granato
Great as Pisana mentioned , my name is Matt Granato, President and chief executive officer of Pulmonary Hypertension Association , discussing the critical role of pulmonary hypertension associations in shaping the healthcare landscape.
I want to emphasize the Pulmonary Hypertension Association Mission to extend and improve the lives of those affected by pulmonary hypertension. and its vision to create a world without pulmonary hypertension, fueled by hope.
I want to start with a little bit of history lesson on Pulmonary Hypertension Association’s recent 30th anniversary and its origins in 1978 when Dorothy Olson, after a challenging diagnosis process, became one of the first patients to highlight pulmonary hypertension.
Her efforts, alongside three other women, led to the creation of the United Patients Association for Pulmonary Hypertension in 1991. This group’s pioneering work, including the distribution of a newsletter, the establishment of support groups, and the creation of a list of pulmonary hypertension -treating physicians, laid the foundation for PHA’s ongoing advocacy, education, and support efforts. From its volunteer beginnings to its current staffed organization, PHA’s growth has been driven by community efforts, fundraising, and innovative initiatives aimed at ending patient isolation and enhancing care for those with pulmonary hypertension.
Today, we stand as a vibrant community at the intersection of patients, caregivers, healthcare providers, and industry partners, united in our fight against pulmonary hypertension. With over 2,200 active members and numerous subscribers, our organization, headquartered in Washington DC, functions as a unique hybrid of an advocacy group and a professional medical society. Our dedicated team of 36 staff members manages a budget of nearly $9 million, enabling us to drive progress and offer support to those affected by pulmonary hypertension.
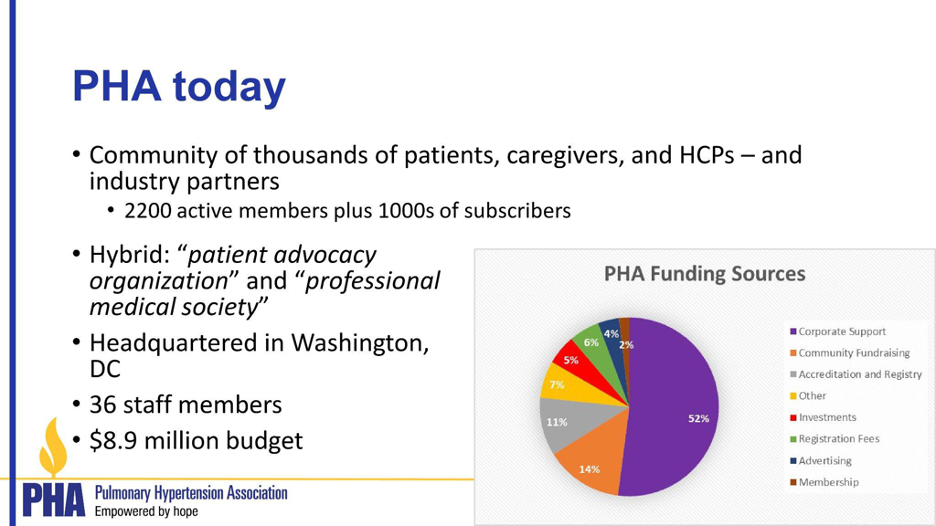
Our journey from humble beginnings to where we are today has been remarkable. The majority of our funding stems from corporate partnerships, with several companies dedicated to developing pulmonary hypertension therapies. The remainder of our financial support comes from community fundraising, accreditation, and a registry program, reflecting the diverse nature of our funding sources.
Our mission remains focused on extending and improving the lives of those impacted by pulmonary hypertension. We achieve this by delivering programs directly to patients or through those who influence their care environment, thereby shaping the care landscape.
Advocacy is a cornerstone of our efforts, aiming to influence government agencies, insurance providers, and pharmaceutical companies to prioritize patient needs.
Additionally, we focus on raising awareness among the public, patients, and caregivers, and on educating healthcare professionals to stay abreast of the latest developments in pulmonary hypertension care. We have patient education programs and we have peer support programs.and finally the medical component as we network several healthcare professionals and institutions that provide medical care in pulmonary hypertension.

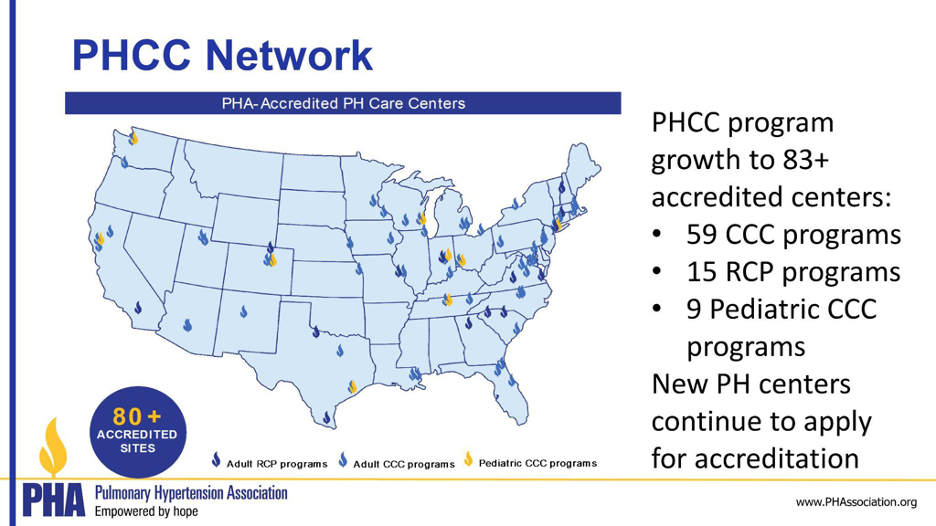
A significant milestone was the initiation of a program to accredit care centers about a decade ago, ensuring a network of centers across the United States that meet minimum standards of care for pulmonary hypertension patients. This accreditation, along with a patient registry, enables us to support research and development of new therapies.
Our advocacy efforts include legislative, regulatory, and judicial initiatives, emphasizing the importance of patient stories in driving change. We strive to influence regulations and laws to improve patient access to care and to strengthen the healthcare professional-patient relationship be it coverage or reimbursement.
To raise awareness, we utilize innovative tools like our publication “Navigating Pulmonary Hypertension” and a patient-centered microsite, Pulmonary Hypertension Association Connect Hub, serving as a one-stop shop for patient resources. Our patient support groups, the largest community of their kind, have transitioned to a blend of in-person and virtual meetings to ensure continued support during the COVID-19 pandemic.
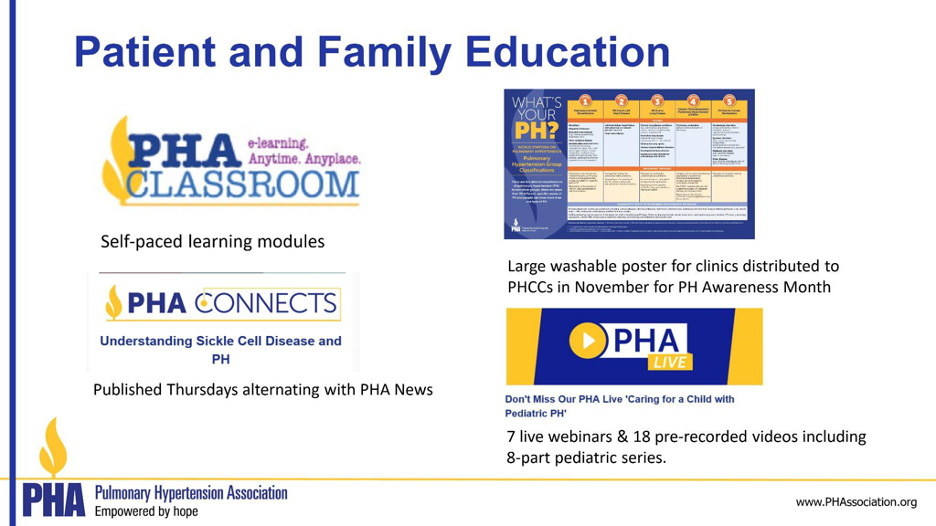
Education remains a key focus, with programs like the Pulmonary Hypertension Association Classroom offering self-paced learning modules and our annual conference providing a platform for sharing the latest scientific developments.
We also offer continuing medical education programs for healthcare professionals, including Pulmonary Hypertension Association Online University and symposiums.
Lastly, our Pulmonary Hypertension Care Centers program accredits over 83 programs nationwide, ensuring quality care for pH patients. Our Pulmonary Hypertension Association registry, a crucial component of this program, supports clinical trials and fosters collaboration among care centers.
In summary, our organization, with over 30 years of experience, is dedicated to advancing the care of pH patients and shaping the care landscape through advocacy, education, and research. Thank you for the opportunity to share our progress and initiatives.
Robert Pleticha
Thanks very much Matt , now the next speaker will be Melanie from HTaP France .
Melanie Gallant-Dewavrin
I’d like to express my gratitude to Matt and the US Pulmonary Hypertension Association for the profound inspiration they’ve provided. Their ambitious program and model stand as a beacon for all, especially smaller associations. I’m eager to share the journey we’ve embarked upon in France with the creation of the French Pulmonary Hypertension Association HTaPFrance
Reflecting on the context of the late 20th century, which has been previously discussed, I bring my own experiences and perspective today. Pulmonary arterial hypertension was first documented in 1891, and by the time we were addressing primary hypertension a century later, it had been recognized at a 1973 conference in Geneva as a rare disease, with the total reported cases and deaths numbering around 100.
Turning to the first reports and historical accounts, we observe the landscape of the 70s and 80s. During this era, pulmonary arterial hypertension was largely unidentified as a distinct disease, often perceived merely as a symptom with a bad prognosis. Diagnostic tools such as echocardiography were not commonly used. Before the 1980s, the primary diagnostic methods were electrocardiograms, X-rays, and catherterism, with treatments limited to calcium blockers and little else..
The first heart-lung transplant, which occurred in 1981. Subsequently, France celebrated its first heart-lung transplant. The pioneering medication, epoprostenol (Flolan), was approved in the United States in 1995 and in France four years later, in 1998.
During a significant meeting in Evian in 1998, the medical community moved away from distinguishing between primary or secondary pulmonary hypertension, adopting the terms PAH (Pulmonary Arterial Hypertension) or associated pulmonary hypertension instead. This shift marked a significant advancement in the field.
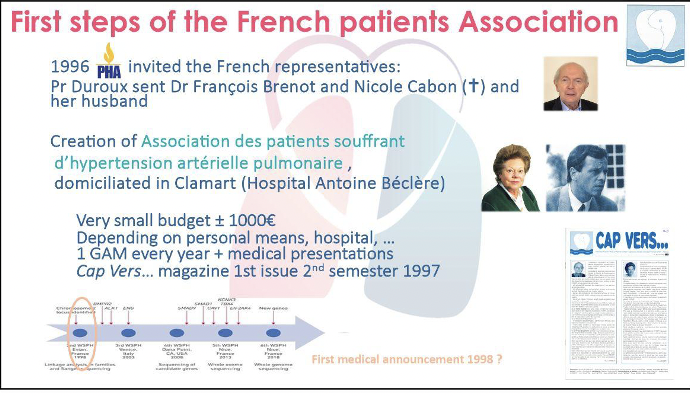
In 1996, French representatives were invited by the Pulmonary Hypertension Association to their conference. Professor Duroux delegated Dr. Francois Brenot, Nicole Cabon, and a patient to attend. The conference was enlightening and inspired the French team. Motivated by their experiences, they promptly established an association in 1996, following the conference. This association, which began with a modest budget of no more than €1,000, was domiciled in the Hospital Antoine Béclère in Clamart, reflecting its close ties to the hospital and its reliance on personal contributions and hospital-based meetings.
The association, housed within the hospital where the French team collaborated extensively. Additionally, they launched a magazine titled “Cap Vers,” which first issued in 1997 and continues to be published, albeit under various names.
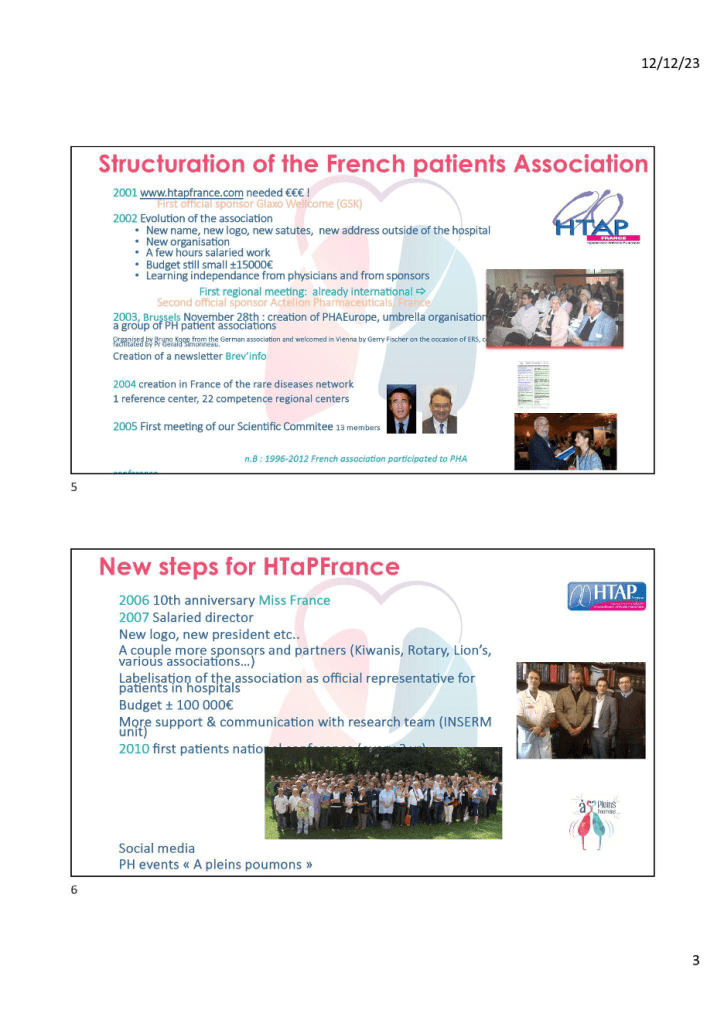
The French Patients Association, known as HTaPFrance, underwent significant structural changes beginning in 2001, which necessitated substantial funding. The first major financial support came from Glaxo Wellcome. By 2002, the association evolved with a new name, logo, statutes, and a relocation from the hospital to a new address. Despite its development, the organization operated on a modest budget of approximately €15,000 and began to establish its independence from physicians and sponsors.
In 2003, the association received sponsorship from Action Pharmaceuticals, France, which became the second official sponsor. That same year, on November 28th in Brussels, the creation of PHAeurope was announced, serving as an umbrella organization for a collective of Pulmonary Hypertension patient groups. Furthermore, 2003 marked the inception of ‘Brev’info,’ a newsletter aimed at disseminating information within the community.
The year 2004 was a milestone for the association with the establishment of France’s rare diseases network, which included one reference center and 22 regional competence centers. In 2005, HTaPFrance held its first Scientific Committee meeting with 13 members. It is noteworthy that from 1996 to 2012, the French association was an active participant in the Pulmonary Hypertension Association.
As HTaPFrance entered a new phase in 2006, they celebrated their 10th anniversary with an event featuring Miss France. The following year saw further developments, including the appointment of a salaried director, introduction of a new logo, and a change in presidency. The association expanded its sponsor and partner base, including Kiwanis, Rotary, Lion’s Club, and various other associations, reinforcing its role as an official representative for patients in hospitals. By 2007, the budget had grown to approximately €100,000, allowing for greater support and enhanced communication with research teams, particularly with a French national institute of health and national research unit. A significant achievement came in 2010 when HTaPFrance organized its first national meeting for patients.
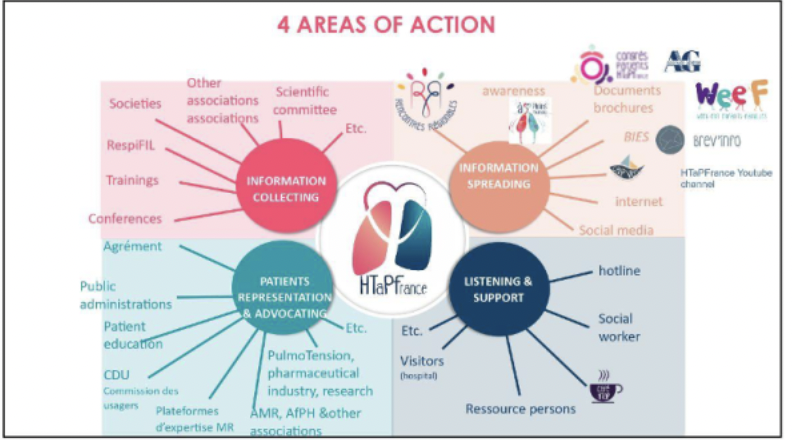
In addition to these advancements, HTaPFrance also embraced social media to reach a wider audience and organized events such as “A pleins poumons”.
In our efforts to support patients and carers, we’ve established a triennial national conference and embraced social media to enhance awareness and fundraising initiatives. However, like any organization, we face challenges such as the need for increased transparency, diversification of funding, and the ongoing difficulty of recruiting volunteers. Professionalism within our operations remains a priority.
Our initiatives, including regional meetings, conferences, and family weekends, aim to build a supportive community. These gatherings, represented by the logos shared, facilitate not only information sharing but also essential social interactions among our community members.
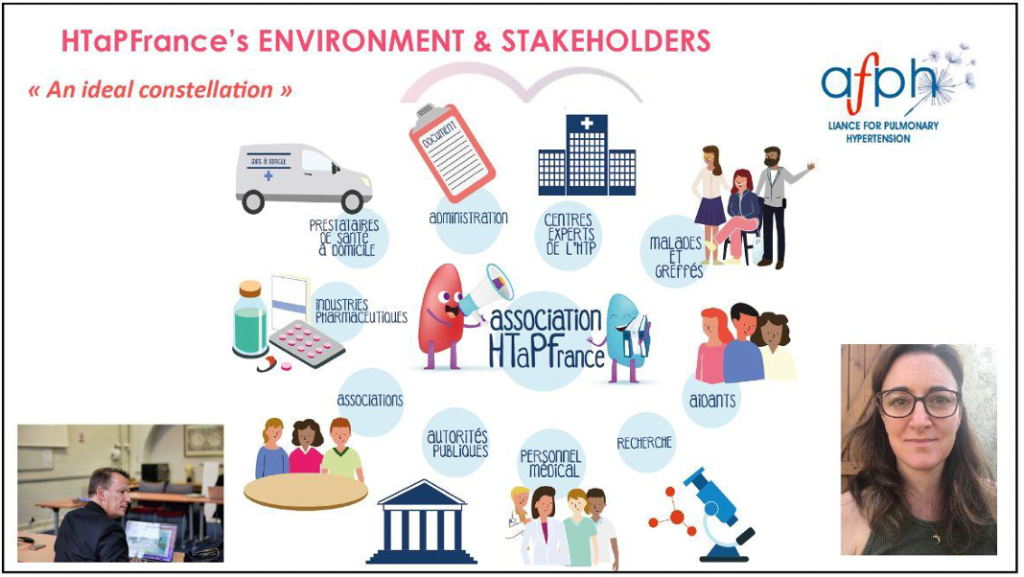
We operate within a network that includes physicians, researchers, pharmaceutical companies, other associations, public authorities, medical professionals, carers, and expert consultants. This collaborative ecosystem is vital for advancing our cause. Professor Humbert, serving as our mentor, exemplifies the strong support system surrounding us and our patient president Maggie Serras,I know she is listening to us now.
Thank you for your attention. I look forward to addressing any questions before we transition to the presentation from the German association’s representative.
Hans Dieter- Kulla
Thank you for allowing me the opportunity to present at this meeting. I am here to share a brief history of a German organization, which was founded in 1996. The foundation was driven by our founder, Bruno Kopp, who was himself a patient seeking treatment options for his disease. During these challenging times, the key locations offering support for pulmonary hypertension were Giessen, Heidelberg, and Bad Nauheim. The pioneers in this field, Werner Seeger, Ardeschir Ghofrani, Horst Olschewski, and Ekkehard Grünig, began treating the condition and remain active contributors to the field.
The initial vision and mission of the organization were centered on patient welfare, aiming to improve their circumstances significantly. Our objectives included making patient care accessible locally, disseminating knowledge about pulmonary hypertension across Germany, involving politicians and decision-makers to enhance the overall situation, and establishing an operational platform to ensure the smooth functioning of our system.
One of our key challenges has been raising awareness about pulmonary hypertension, its causes, and its implications, as it is not widely recognized. We also focused on bringing together physicians, the industry, and patient groups to foster collaboration. To this end, we host an annual patient meeting in Frankfurt, where experts discuss new medications, techniques, and developments, and patients share their experiences, which has proven to be immensely beneficial.
In terms of development milestones, we initially formed an Advisory Board composed of 14 physicians to assist with general inquiries. Following that, in 2006, we launched specialized training programs for nurses to enhance their understanding of diseases due to their proximity to patients. Another significant step was supporting research through an annual award for the best publication, promoting advancements in the field.
Over the past decade, as President of various German organizations, I’ve witnessed significant advancements in the clinical development field. The introduction of new treatments has markedly improved, offering enhanced support and quality of life for patients. We’ve successfully conducted clinical trials yielding positive outcomes and, since last year, implemented new guidelines that standardize care globally. Our association initiative has been instrumental in fostering knowledge sharing about the disease, furthering our understanding and ability to manage it effectively. Research in genetics has opened new avenues for patient care.

Our organization boasts around 1,300 members in Germany, with 98% contributing on a voluntary basis. We maintain a paid office staff to ensure operations run smoothly throughout the week. This structure has been crucial in our efforts to advance national and international collaboration. Despite the current inability to cure the disease, our work has led to the development of new drugs and a deeper understanding of the condition, significantly improving patient life expectancy and quality.
The emphasis on global knowledge exchange remains a cornerstone of our mission, as we strive to support and enhance patient care. I hope this overview provides insight into our achievements and ongoing endeavors. Thank you for your interest and any questions you may have.
ROBERTA PLETICHA
Thank you very much, Peter. It’s encouraging to see the evolution of the German patient group. Pisana, I believe you’re set to provide a summary next.
PISANA FERRARI
We’re short on time, so I’ll quickly highlight our progress from no patient associations before the 1990s to over 90 today across six continents. This shows significant progress, though some areas still lack adequate support. Many thanks to the US Pulmonary Hypertension Association for their map, which illustrates the broad and varied landscape of patient care and support. Organizations offer resources and connections at all levels, with forums, social media, and new informal groups enhancing support. However, support quality varies due to several factors, including economic and geographic conditions. Some regions still lack patient associations, a gap partially bridged by online connectivity where possible.
Importantly, patient associations have evolved to include awareness, advocacy, and participation in healthcare decisions, with groups and associations leading the way. Gergely will next provide an overview of these developments.
Thank you for your attention.
GERGELY MESZAROS
Many thanks again for having me, and welcome to everyone who joined us this evening to learn a bit about history.
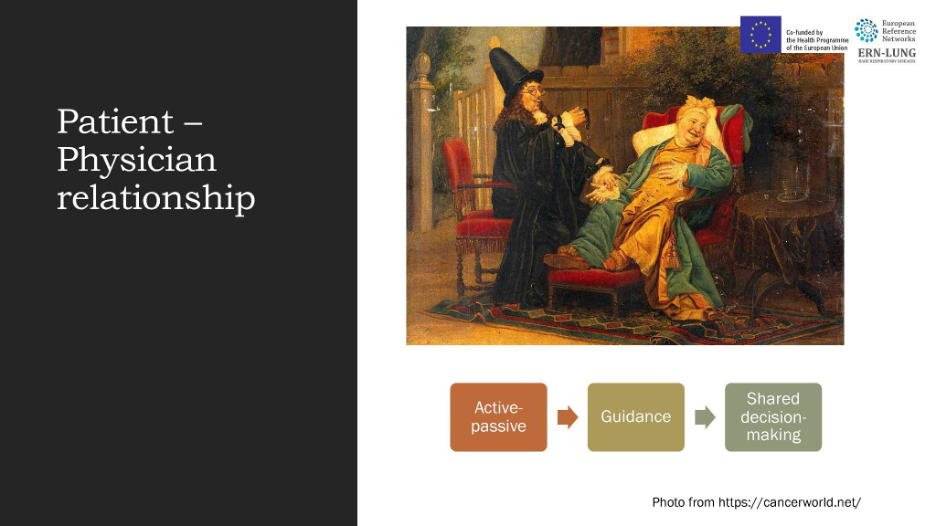
However, I won’t be discussing history extensively, as there was already a comprehensive review. Instead, I’d like to focus on some points I believe are important, particularly how the patient-physician relationship has evolved. Initially, this relationship was active-passive, then moved to guidance, and now we are in the phase of shared decision-making, as reflected in the new guidelines.
If we examine the relationships between patient associations, physicians, and the global and wider communities, we find distinct stages worth exploring. I’m not focusing on the pulmonary hypertension association specifically, but rather on a broader perspective. The first self-help group was established in the 1940s, and by the 1960s, combating stigmatization became a primary advocacy goal for these associations. Modern advocacy began in the 1980s and 1990s. We’re discussing patient associations today because the latest pulmonary hypertension guidelines include, for the first time, a separate section on patient associations and information, with a clear recommendation for pulmonary hypertension centers to collaborate with them.

Skipping the definition of patient associations for now, it’s worth noting they are typically nonprofit organizations led mainly by patients. There’s room for discussion on improving these standards, which we might cover later in the discussion section. Pulmonary hypertension associations play a crucial role in enhancing patient quality of life through advocacy, a key focus area.
However, the landscape for pulmonary hypertension associations is complex. First, let’s discuss connections to European scientific societies, starting with the European Reference Network for Rare Respiratory Diseases, ERN-Lung. Though primarily consisting of healthcare professionals, it offers a platform for patient interaction through a Patient Board that participates in the main decision-making body, the Medical Steering Committee. Notably, major umbrella associations like Pulmonary Hypertension Association Europe, PHA EUROPE, are represented at the highest level.
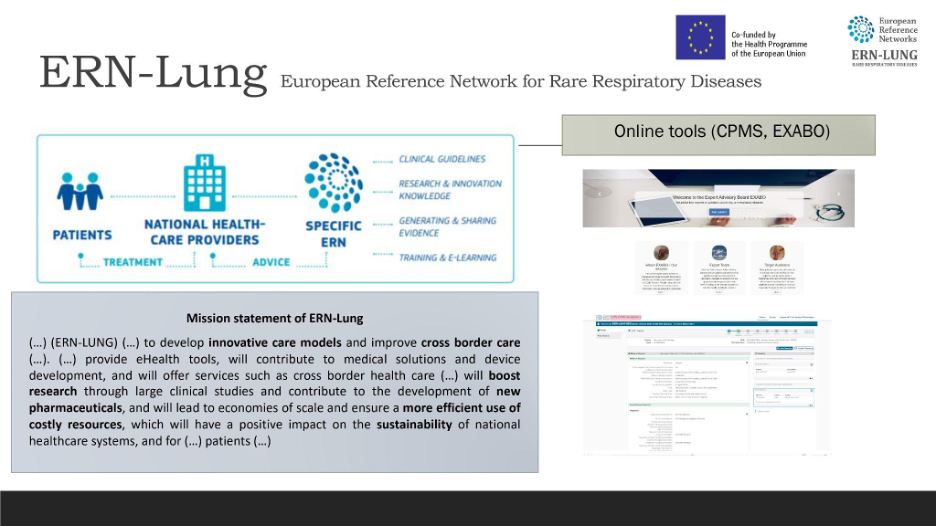
European Reference Network for rare respiratory disease aims to enhance cross-border healthcare, contributing to innovative care models and building a more effective system where knowledge travels, not patients. This is facilitated by online tools, panels, and second opinions that improve healthcare delivery.
Another important platform is the European Lung Health group, which has collaborated extensively with Pulmonary Hypertension Association Europe.

This collaboration focuses on common themes across respiratory associations, both rare and common, and was established in 2020. Its main activities involve connections with World Health Association, the European Parliament, and the European Commission, and include a special group of European Parliament members, there’s a need to restart certain projects and initiatives under this group, including the European Patients Forum (EPF), which aims at foresight into future healthcare.
In conclusion, raising awareness and advocating for respiratory health are crucial, as demonstrated by the recent key prepping project launched at the European Respiratory Society meeting in Milan.
This project, developed amid the Corona pandemic, centered around a research theme supported by a group attended by members of the European Parliament. Key to this initiative was the partnership with the European Respiratory Society , a significant ally, which fostered collaboration and ensured patient involvement across various task forces, notably in clinical research collaborations. This initiative marked a pioneering effort by the European Respiratory Society and our physician partners in pulmonary hypertension to include patients and patient advocates in developing guidelines and contributing to papers, such as the statement on chronic thromboembolic pulmonary hypertension, alongside other significant works.
Further, we were invited, along with Pisana, to share insights on patient life under COVID-19 restrictions as part of the European Respiratory Society vision. The project also engaged with the European Society of Cardiology, reflecting the interdisciplinary approach to treating pulmonary hypertension, given the different roles of cardiologists and pulmonologists across countries.
A recent webinar highlighted our collaborative work with the European Society of Cardiology on quality indicators, a subject gaining increasing attention. Despite a closer working relationship with the European Society of Cardiology and European Respiratory Society, other scientific societies were also engaged, albeit to a lesser extent. The European Society of Cardiology’s Patient Forum and the European Respiratory Society ’s European Lung Foundation were instrumental in facilitating patient contributions to scientific discussions, with initiatives like the European Patient Advisory Programme and the Patient Advisory Group playing pivotal roles.
The European Society for Organ Transplantation notably advanced patient involvement by welcoming patients to their annual congress, a move echoed by the European Transplant Patient Organisation.
The focus then shifted to the World Symposium, emphasizing ongoing developments in pH guidelines and the inclusion of patient perspectives from the outset.

Lastly, the discussion highlighted the European Medicines Agency’s role in incorporating patient views into regulatory processes, underscoring the importance of patient representation in scientific committees and the broader impact of patient advocacy on healthcare policies, as evidenced by the work of the European Rare Disease Organisation and the European Patients Forum.
This narrative underscores the significant strides made in integrating patient perspectives into healthcare research, policy, and practice, emphasizing the collaborative efforts of various organizations and the potential for future advancements.
Several challenges and opportunities within this field merit discussion, though I will not delve into details at this moment. I’ve presented these on the screen and would now like to open the floor for any questions or comments you might have. There may be particular interest in the challenges we face, and I also have additional information on opportunities. Thank you for your kind attention.
ROBERT PLETICHA
Thank you, Gregory. We have a question: What is required for a patient association to evolve from primarily focusing on advocacy to engaging as a medical entity? Specifically, how can patient groups make the shift from advocacy to active medical involvement? I assume forming a medical advisory board would be a component of this transition, correct?
GERGELY MESZAROS
Our position is notably strong, drawing insights from the US Pulmonary Hypertension Association, which is transitioning towards medical endorsement of centers. To address the question before passing it to Matt, the transition hinges on the vision and mission held by the leadership of patient associations. There’s a significant scope for these associations to contribute to and engage in policy work. For example, the current revision of rare disease plans across various countries presents an excellent opportunity for patient associations to gain visibility at the local level. Additionally, collaborations with entities like the European Lung Foundation’s Patient Advisory Group and other respiratory health initiatives offer avenues to connect, contribute, and influence the future landscape of healthcare.
Matt Granato
To enhance our organization’s initiatives, the crucial first step was to ensure access to leading medical experts and offer them a chance to volunteer with us, which led to the formation of the Scientific Leadership Council. This council consists of experts, predominantly physicians but also including a variety of healthcare professionals such as nurses, registered nurses, physician assistants, and nurse practitioners. These experts began utilizing their knowledge and resources to create specialized educational materials. This initiative was particularly vital, as there is no specific association or medical society in the United States dedicated to pulmonary hypertension; education was primarily aimed at cardiovascular diseases broadly, with no focus on pulmonary hypertension. Our organization successfully filled this gap, establishing ourselves as a hybrid entity that serves both as a patient advocacy organization and, in part, as a medical society for pulmonary hypertension practitioners. This was made possible by harnessing the expertise and willingness of these professionals to volunteer and contribute. Therefore, assembling this network of experts is foundational, enabling us to progress and expand our offerings in pulmonary hypertension care and support.
ROBERT PLETICHA
Thank you, Matt. Before we conclude, I’d like to ask if there are any questions among the panelists. If not, I want to extend my gratitude to everyone for their insightful presentations and for sharing their expertise. We’re excited about the prospect of sharing all these valuable contributions—videos and slides—on our knowledge sharing platform very soon. Please ensure you check there for updates and also follow the PH Alliance on LinkedIn and Facebook to stay informed about our upcoming initiatives. We’re looking forward to connecting with you next year. Until then, take care.