
“LUNG AND HEART-LUNG TRANSPLANTATION IN PULMONARY HYPERTENSION”, MARCH 18, 2024
NB. This transcript can be translated into your preferred language – use orange button at the bottom centre of this page to select it (slides are not translatable).
DISCLAIMER: Despite every effort to ensure the accuracy of this transcript, we strongly encourage all visitors to consult with their healthcare professionals before making any decisions based on the information provided. Additionally, while the quality of Google Translate has improved tremendously in recent years, please remember that it is an automated service and not a human translation.
PROF. LAURENT SAVALE
First, it is important to remember that the development of medical therapies for pulmonary hypertension has considerably improved the prognosis, symptoms, and quality of life, but that pulmonary hypertension remains an irreversible disease.
Consequently, lung transplantation remains an important treatment option for patients with pulmonary arterial hypertension refractory to optimized medical therapy. And to go further, a project of transplantation should be considered at an early stage in the patient’s care because it remains an ambitious and challenging project which can only be planned if all the conditions are met. That’s what we’re going to discuss now.
Briefly, few data from registries are available on the epidemiology of transplantation in pulmonary hypertension are available. I reported here a recent analysis from the French registry performed over the last 10 year period. Only 5% of patients aged under 65 have received a lung transplant or a heart-lung transplant during this period.

And if we analyze the transplant registries, pulmonary arterial hypertension never represents more than 8% of indications for lung transplantation.
Access to transplantation remains challenging for different reasons but it’s a project that should be a source of hope for the patients with severe pulmonary arterial hypertension and who are potential candidates.
It’s challenging for different reasons:
- First, as I said previously, patients with pulmonary arterial hypertension are representing a small proportion of transplanted patients and lung transplantation in pulmonary arterial hypertension requires a highly specific intra- and post-operative strategies. This point will be detailed by the next presentation.
- Second point. The prognostic parameters for risk assessment on list and postoperatively in pulmonary arterial hypertension are very different from the other indications for LT that can lead to inequities in the organ allocation process.
- In severe forms of pulmonary arterial hypertension, there is a risk for developing short-term life-threatening complications (acute decompensated pulmonary hypertension) needing priority access to transplantation.
- Need for heart-lung transplantation in specific cases that can complicate the access to transplantation.
But it is important to underline that for all these specific aspects, there are now solutions that can be proposed and advances that have been made or are being developed to optimize access to transplantation for pulmonary arterial hypertension.
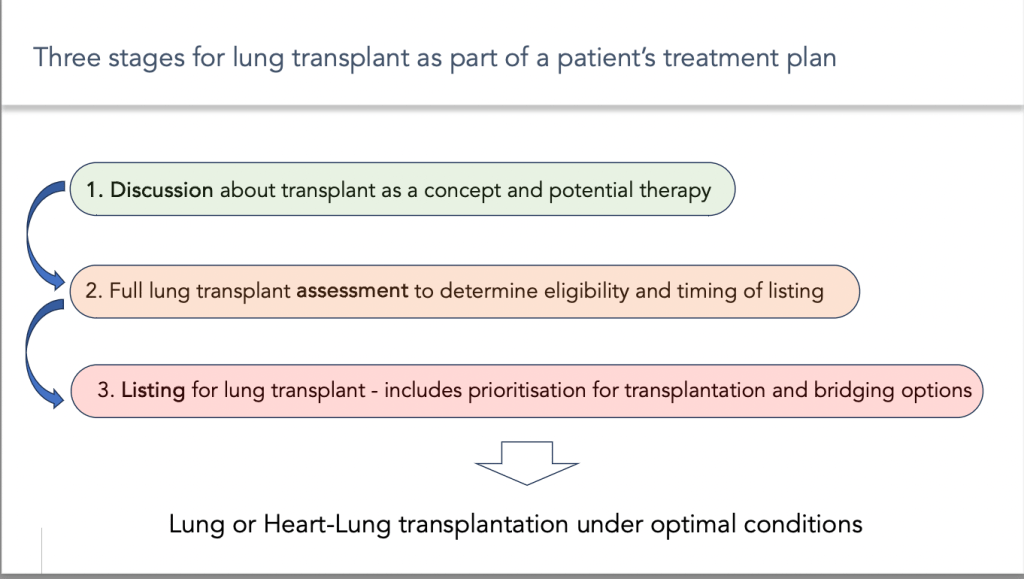
One key point is that the transplant project should be considered at an early stage in the patient’s care, and should be carried out in several stages:
- The first step is the time for discussion about transplant as a concept and potential therapy
- The second step corresponds to the lung transplant assessment to determine eligibility and timing of listing.
- The last step is listing for lung transplant – including prioritisation for transplantation and bridging options.
And it’s important for the medical team to determine the best timing for each of these steps according to the evolution of the disease and according to the specific context for each patient.
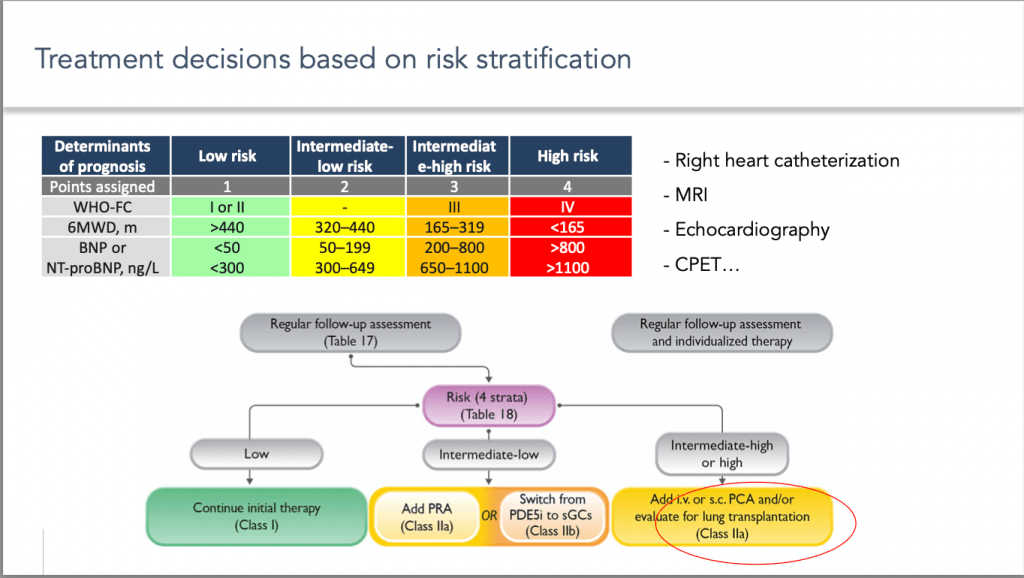
As you know, the treatment algorithm for pulmonary arterial hypertension is essentially mainly on risk stratification during follow-up, using a multi-parametric approach. The aim of this risk stratification is not only to set therapeutic goals, but also to detect patients who are not responders of treatment to consider transplantation when treatment is at its maximum level.
But what is important to underline is that these risk stratification tools should not be used in isolation to inform when to refer a patient for transplantation. Pulmonary hypertension is a group of conditions whose prognosis may be influenced by other parameters that should be included in the decision:
- Associated conditions and comorbidities
- Quality of life.
- Some of conditions requires Heart-Lung transplantation that will complicate access to transplantation.
- Outcomes can be also influenced by specific complications.
In addition, to assess the best timing for transplantation, it is important to consider the parameters that will influence the waiting time.
- The size.
- The blood group.
- The HLA sensitization.
- Country related factors.
Taking all these parameters into account, the first question is “When should we talk about transplantation as a concept and potential therapy?”
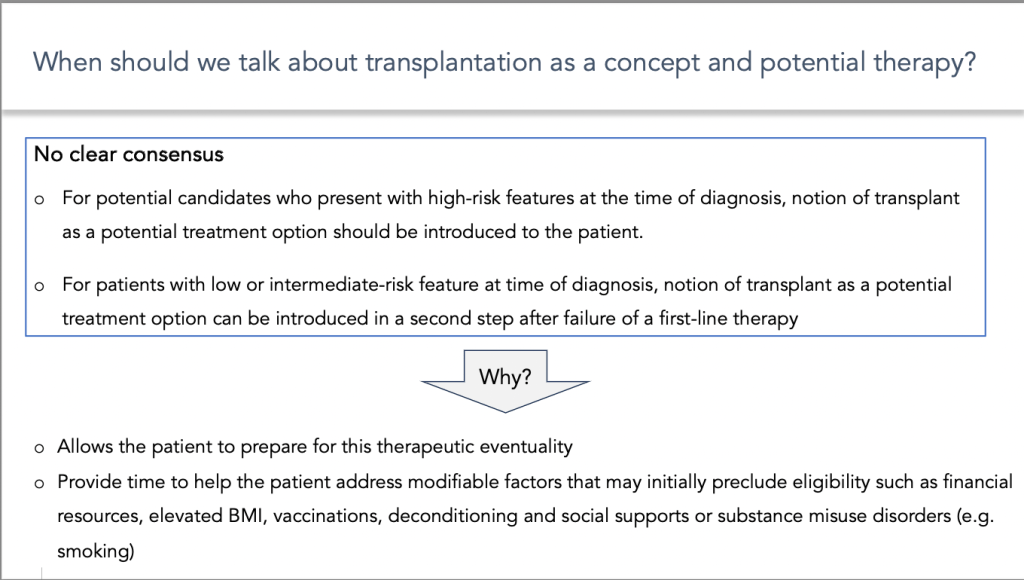
There is no clear consensus on when transplantation as a concept should be discussed with the patient.
This depends on the severity of the underlying disease and the patient’s expectations.
- I think it is reasonable to say that the notion of transplantation should be introduced to patients as soon as the diagnosis is made, when the status is severe and requires maximum treatment as first line therapy.
- When the risk status at baseline is low or intermediate, notion of transplant as a potential treatment option can be introduced in a second step after failure of a first-line therapy. This must be adjusted on a case-by-case basis.
Why it is important to introduce early to the patient the concept of lung transplantation:
- First because it allows the patient to prepare for this therapeutic eventuality. A transplantation project can only be envisaged if the patient fully agrees to it and that he feels ready for it. This can sometimes take time.
- Secondly, it allows providing time to help the patient address modifiable factors that may initially preclude eligibility such as financial resources, elevated Body Mass Index (BMI), vaccinations, deconditioning and social supports or substance misuse-related disorders.
The second time is the lung transplantation assessment to determine eligibility
Once again, the decision to refer for transplant assessment should be based on different parameters.
It can be carried out at the time of diagnosis if there is a variant of the disease that responds poorly to treatment. It is the case of:
- PVOD, Pulmonary Veno-Occlusive Disease
- Pulmonary arterial hypertension due to scleroderma with venular involvement and/or associated extensive pulmonary fibrosis.
- Severe pulmonary hypertension World Health Organization group 3
During follow-up referral for transplantation should be discussed if:
- Patients at intermediate-high risk or high risk after a first line oral therapy needing parenteral prostacyclin (PGI2) analogs initiation.
- Patients who don’t reach low-risk status after a first line triple therapy including parenteral prostacyclin (PGI2) analogs.
- Significant right ventricle (RV) dysfunction despite optimal medical therapy.
Finally, in case of specific at risk conditions:
- Episode of acute decompensated pulmonary hypertension requiring hospitalization
- Onset of new atrial arrhythmia
- Recurrent non severe hemoptysis
Of course, all these proposals must be modulated according to the medical environment, the healthcare system and other conditions.
This time of screening procedures has different objectives:
First to meet the transplant team in charge of the lung transplant process including Surgeons, Medical doctors, Anesthesiologists, psychologists, transplant coordinator, social workers
The second objective is to screen absolute or relative contraindication for lung transplantation. I listed some of them in the right of the slide. These contraindications are related to:
- Acceptance of transplant program by the patient of course
- Other severe organ failures
- Infection
- Cognitive impairment
- Malignancy
The next step is to determine the type of transplantation
- Bilateral lung transplantation (BLT) is the preferred option.
- Heart-Lung transplantation (HLT) only in specific selected cases:
- Non-correctable cardiac conditions.Coexisting left sided heart disease.
- PA aneurysm or massive cardiomegaly
- In some patients with interstitial lung disease and chronic obstructive pulmonary disease (COPD) or emphysema and mild pulmonary hypertension, single lung transplantation may be sufficient.
With all these information, the medical team determine eligibility and timing for transplant but the final decision should be jointly made between the patient and medical team after informing of the risks and benefits
Once the project has been validated, it is not necessarily the right time for listing but all has been anticipated if there is a progression of the disease.
The decision to listing will depend on the risk and the therapeutic pressure.
During follow-up according to the risk status:
- High risk category despite optimal medical therapy.
- Persistent intermediate high risk with significant right ventricle dysfunction, recurrent hospitalization for right ventricle failure despite optimal medical therapy.
- Liver or kidney dysfunction
Specific high-risk conditions
- Worsening in hypoxemia or hemodynamics in PVOD patients
- Diagnosis of underlying Interstitial Lung Disease (ILD), Chronic Obstructive Pulmonary Disease (COPD), or Combined Pulmonary Fibrosis and Emphysema (CPFE).
- Long waiting times expected on list.
As I said earlier, decisions to refer or list must be modulated according of the care system and the rules for allocating grafts, which can be very different from one country to another.
You have here the example of the heterogenicity of program in Europe.
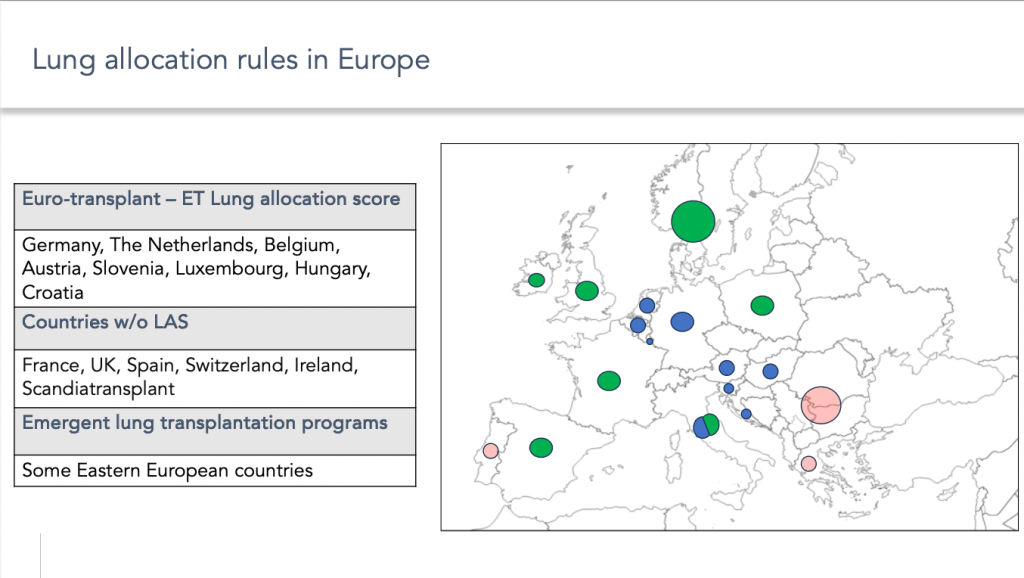
Some countries use graft allocation scores, while others do not.
Finally, in some countries, transplantation programs are still underdeveloped, which complicates access to transplantation for patients with pulmonary arterial hypertension.
Just a word about the pulmonary arterial hypertension in the lung allocation score and how its score has been modified in the United States to improve access to transplantation for these patients.
As I said earlier, the parameters for assessing the severity of pulmonary arterial hypertension are very different from those for other respiratory diseases, which has led to a clear inequality of access to the transplantation with the first LAS implemented in 2005. This was clearly improved after the 2015 changes, which added new parameters specific to pulmonary arterial hypertension and gave more weight to the aetiology itself.
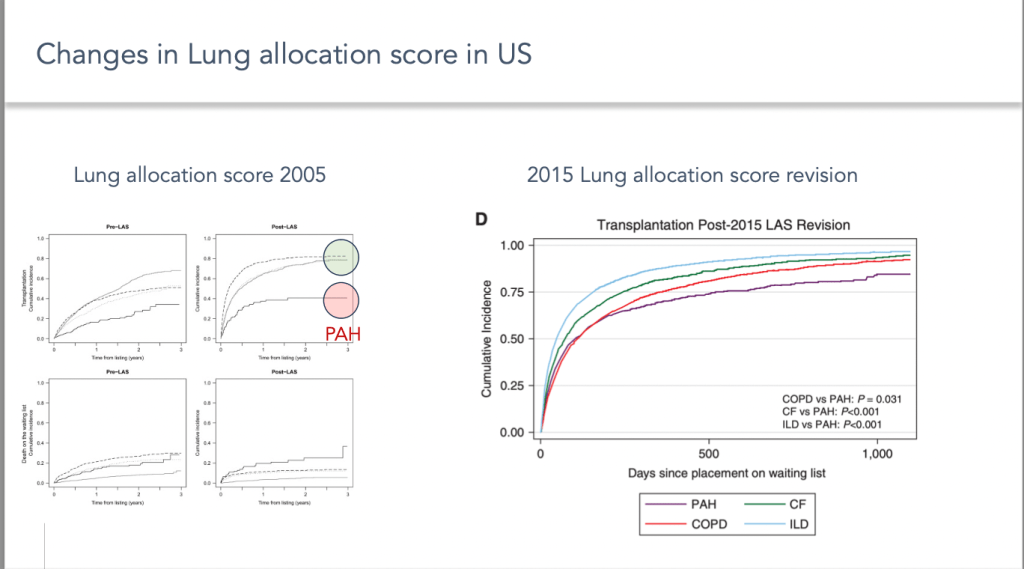
Nevertheless, despite the significant improvement, pulmonary arterial hypertension remains one of the aetiologies for which access to the transplantation remains the most challenging.
Since 2023, the lung composite allocation score was implemented with several changes that could be interesting for pulmonary arterial hypertension patients, but this should be properly evaluated.
Lung allocation scores represent now 50% of the overall score => 50% dependent on the recipient candidate’s biology that influence the expected time on list.
Another major advance has been the gradual introduction of systems allowing urgent access to transplantation for pulmonary arterial hypertension patients in the vast majority of lung transplant programs.
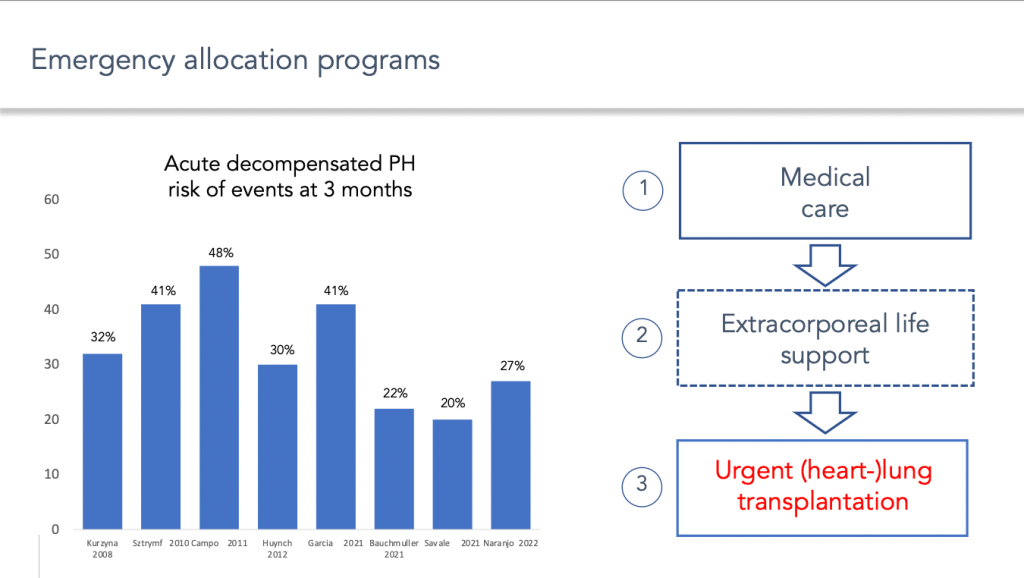
Indeed, patients with end-stage pulmonary arterial hypertension are at risk of developing episodes of acute decompensation of right ventricular failure, which can be life-threatening in the short term. The management of these acute episodes of decompensation has improved considerably, not only with the development of circulatory assistance systems, but also with the development of systems of priority access to transplantation in most severe conditions.
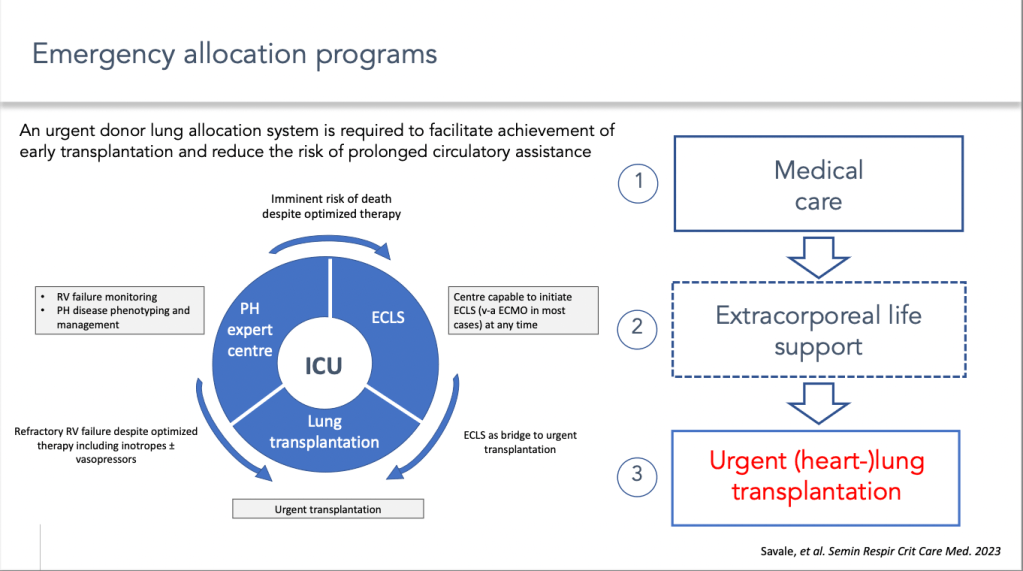
The implementation of these systems means that patients treated for an acute episode of decompensation of pulmonary hypertension and who are candidates for an emergency transplant can be referred to an environment that provides access to all these therapeutic approaches.
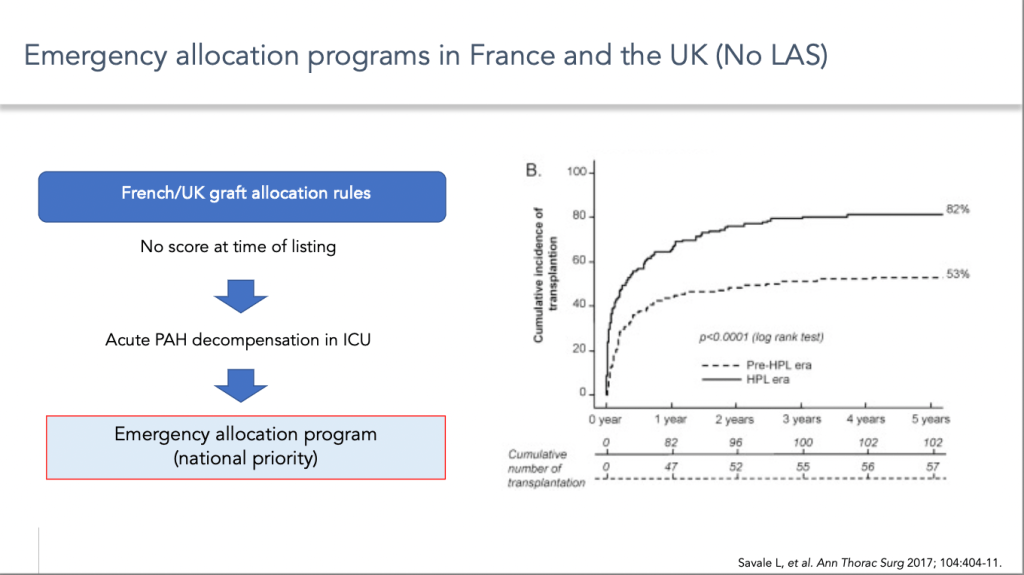
Taking France as an example, the introduction of this system of priority access to transplants has considerably reduced the risk of mortality on the list and therefore considerably improved access to transplants for patients with pulmonary arterial hypertension.
To conclude:
- Access to transplantation for pulmonary arterial hypertension remains challenging, with a wide variability depending on the healthcare system and the graft allocation rules.
- Evaluation of a lung transplant program should be considered at an early stage in the treatment algorithm
- Patients be engaged in discussions about transplantation as a treatment option early in their treatment course.
- Final decision should be jointly made between the patient and medical team.
- Decisions to refer and then list patients should be comprehensive and include risk assessment, comorbidities, anticipated wait list times and donor pool.
- Development of urgent transplant program