
- Dr Julie Wacker Download the slides
- Prof Maurice Beghetti Download the slides
- Katleen Verbergt Download the slides
Transcript “CONGENITAL HEART DISEASE AND PULMONARY HYPERTENSION”, MAY 18, 2024
NB. This transcript can be translated into your preferred language – use orange button at the bottom centre of this page to select it (slides are not translatable).
DISCLAIMER: Despite every effort to ensure the accuracy of this transcript, we strongly encourage all visitors to consult with their healthcare professionals before making any decisions based on the information provided. Additionally, while the quality of Google Translate has improved tremendously in recent years, please remember that it is an automated service and not a human translation.
ROBERT PLETICHA, MODERATOR
Hello, everyone, and welcome. This is the third webinar of 2024 by the Alliance for Pulmonary Hypertension. If this is your first time at one of our webinars, the Alliance is a nonprofit organization registered in Brussels whose mission is the sharing of knowledge and expertise about Pulmonary Hypertension.
My name is Rob Pleticha. I’m from admedicum, and we’ve had the pleasure of assisting the Alliance for Pulmonary Hypertension for the last three years. Today, our esteemed medical speakers, Dr. Julie Wacker and Professor Maurice Beghetti, will talk about congenital heart disease and pulmonary hypertension. Then we’re very excited to have Kathleen to share the experience of being a mother of a young person living with the condition. So, as always, questions can be submitted in the chat box wherever you’re watching this, and we’ll collect those and ask them at the end. The recording and the slides and transcript will be available on the knowledge sharing platform in the next few weeks.
The next webinar is on June 18th, and it will be about the genetics of pulmonary hypertension. Without any further delay, let’s get to today’s topic, which is congenital heart disease and pulmonary hypertension. Dr. Wacker, would you like to take the stage, please?
JULIE WACKER
I’m a pediatric cardiologist at the Geneva University Hospital, and I’m very pleased to talk to you about congenital heart disease and pulmonary hypertension.

So, as you know, congenital heart disease can occur in about 1 to 100 live births, and about 4 to 28% of patients born with a congenital heart disease will develop pulmonary hypertension.
I’m going to talk a bit about physics, so bear with me. I’m going to try to make it very simple.
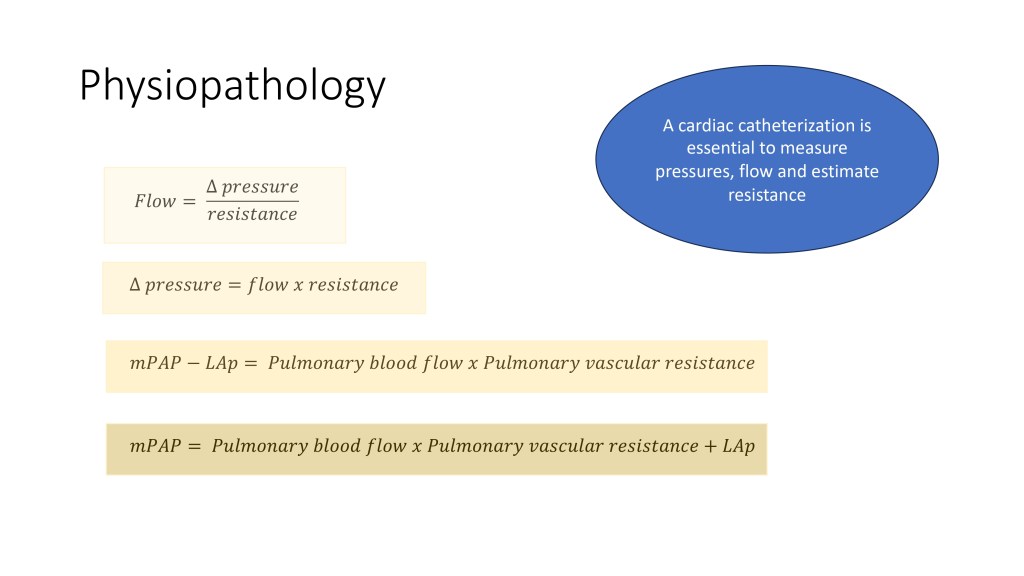
As you may know, a flow through a circuit is the ratio of the difference of pressure in that circuit on the resistance. And if we move that equation around, the different data of pressure is the flow times the resistance. And when we apply that to the pulmonary vasculature, we can see that the mean pulmonary artery pressure minus the left atrial pressure, which is the delta flow across the pulmonary vascular bed, is the pulmonary blood flow times the pulmonary vascular resistance.
We move that around a little bit more, and we have the mean pulmonary artery pressure (PAP), which is necessary for the definition of pulmonary hypertension, and which is the pulmonary blood flow times the pulmonary vascular resistance plus the pressure in the left atrium. It is very important to understand how congenital heart disease can lead to pulmonary hypertension. Of note, we need a cardiac catheterization to measure the pressures, to calculate the flow and estimate the resistance in patients.
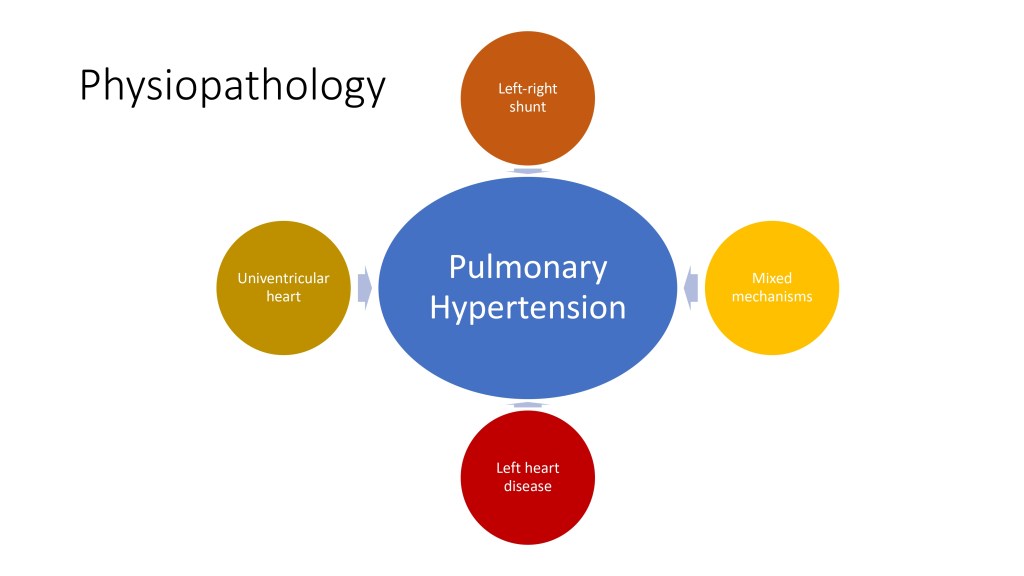
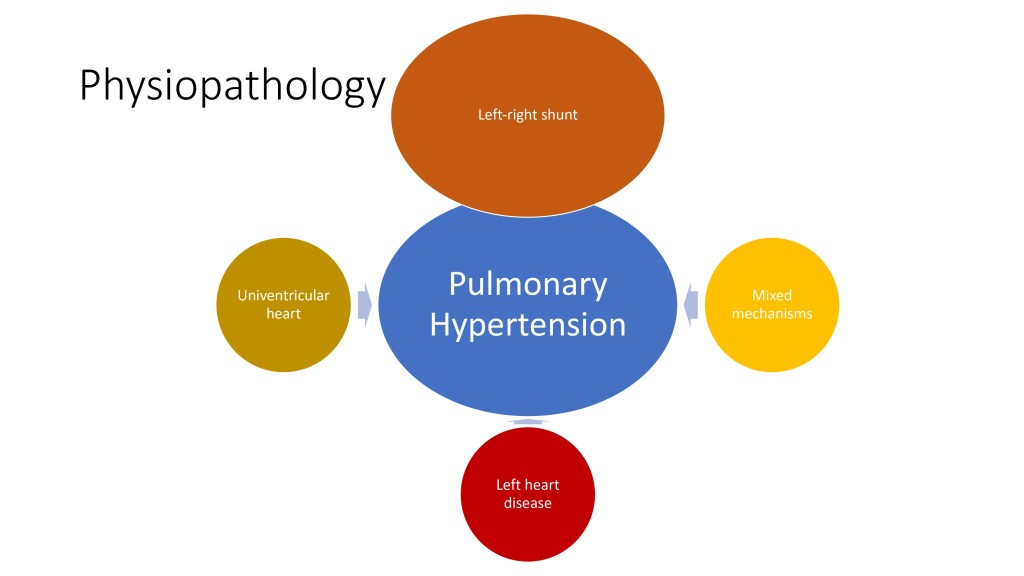
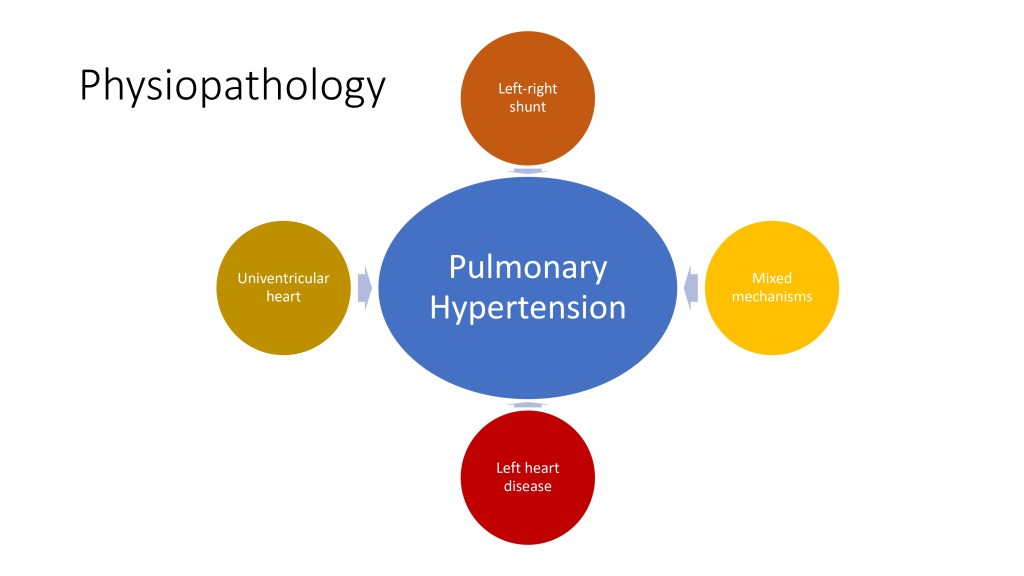
There are many different ways through which congenital heart disease can lead to pulmonary hypertension, and I will describe them in this presentation.
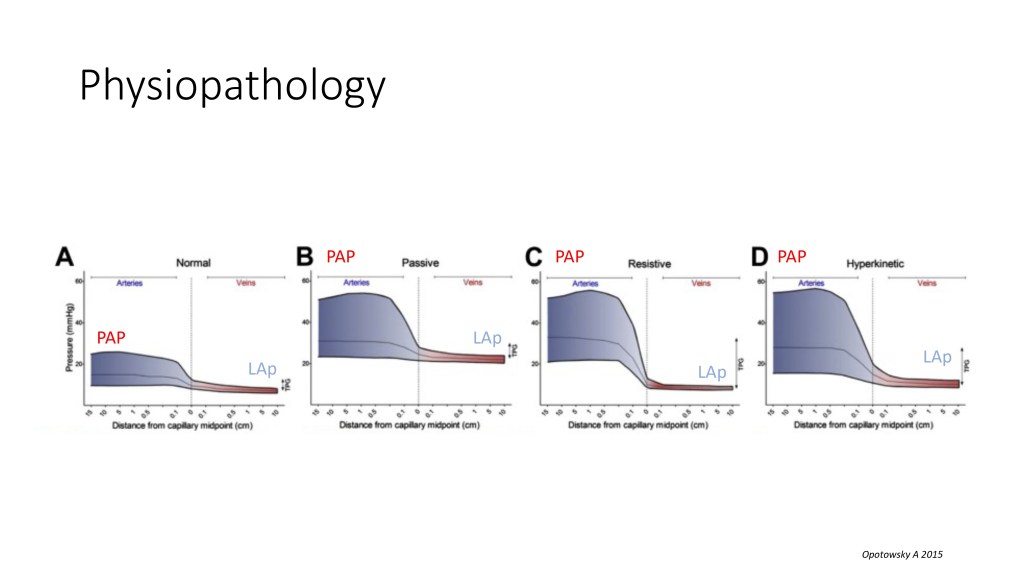
This is a bit of a, just to give you an idea of the delta pressure across the pulmonary vasculature. We have the mean pulmonary artery pressure on the left side of those situations, and the left atrial pressure on the right side.
And you can see that in a normal situation, there is a slight drop of pressure across the pulmonary vasculature. But you can have sometimes, and we’ll see that in the left-sided heart disease, an increase in diastolic pressure and just a passive transmission of this increased pressure on the pulmonary arteries. But sometimes, like in hyperkinetic pulmonary hypertension, like in shunts, and we’ll see that just in a short while, you can have a left atrial pressure that is not very elevated, but the drop of pressure is very impressive inside the pulmonary vasculature because of the increased resistance.
So now we’re going to talk about the left-to-right shunts. In a shunt the blood goes always from where the pressure is higher to where the pressure is lower.
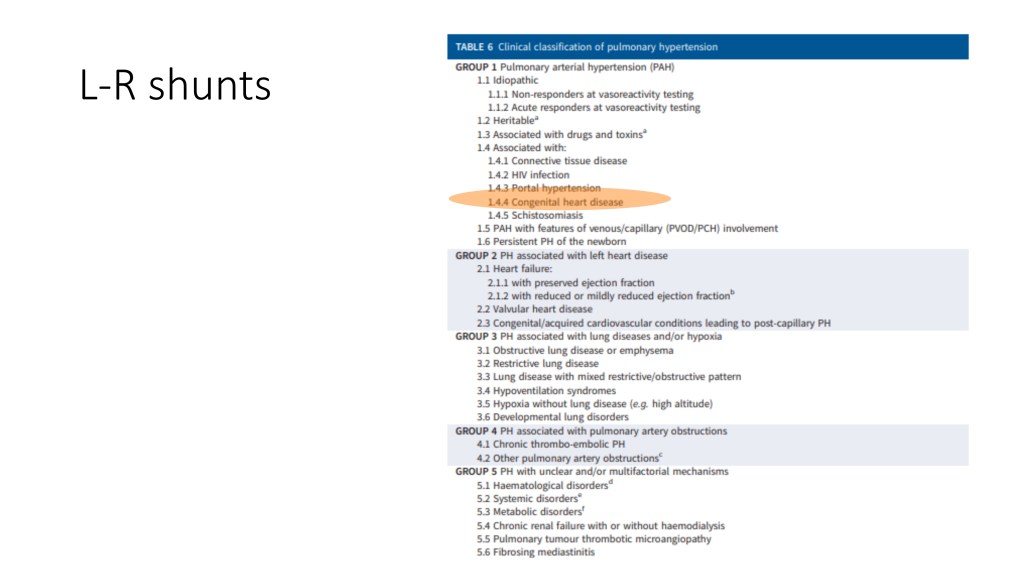
And when we talk about pulmonary hypertension associated with congenital heart disease, and this is the case in the classification of Group I of the WHO classification, pulmonary arterial hypertension, we mainly refer to patients with a left-to-right shunt.
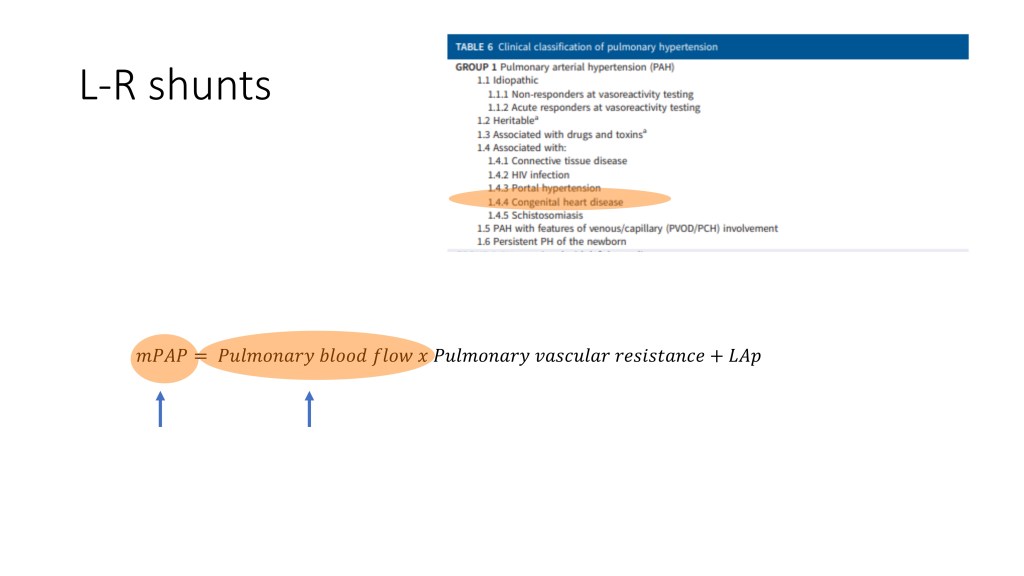
In this situation, you can see that the increase of mean pulmonary arterial pressure is mainly due to an increase of pulmonary blood flow because of all this flow that goes from the left to the right and back into the lungs.
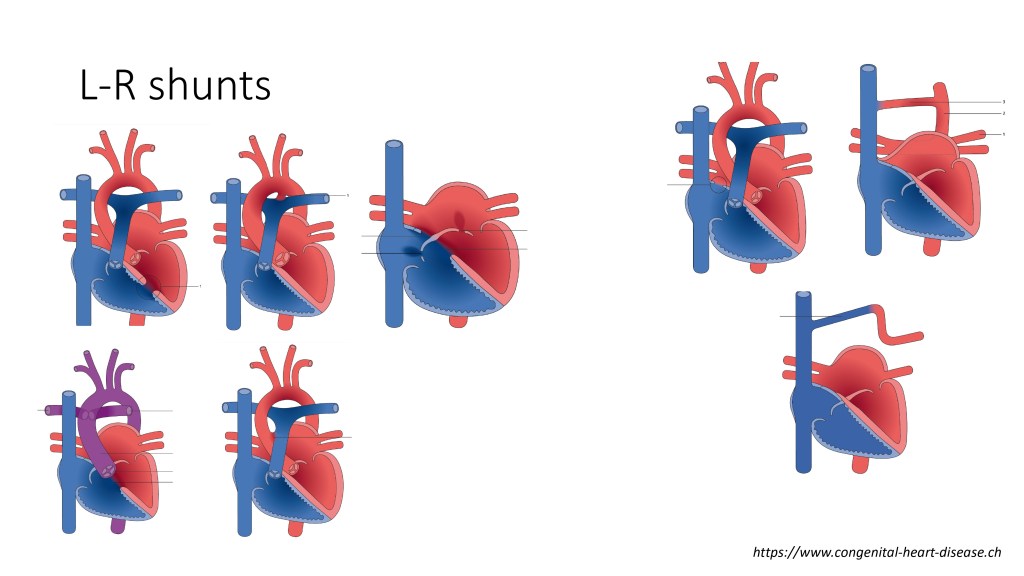
There are many different types of congenital heart disease that can cause pulmonary hypertension, that have a left-to-right shunt. You have the shunts in atrial septal defect, you can have abnormal pulmonary venous drainage, and you can have ventricular septal defects, patent ductus arteriosus, and atrioventricular septal defect, truncus arteriosus, and many other complex diseases that are not all highlighted in this slide.
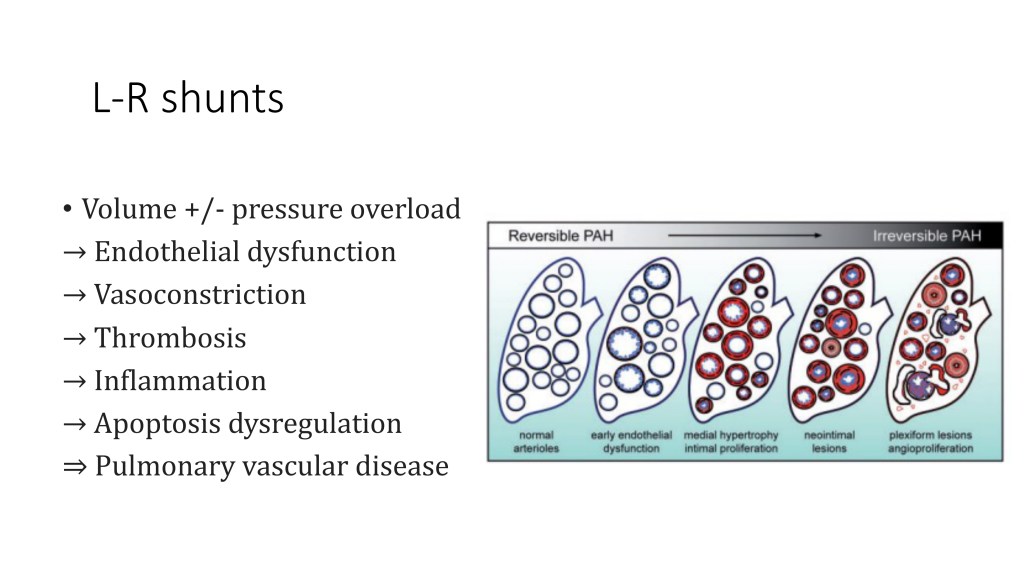
I’m not going to talk in detail about the mechanism by which this increased pulmonary blood flow will lead to pulmonary hypertension in terms of the histological changes. But you can see that at the beginning, you have the arterioles that are normal, and with the increase of pulmonary blood flow, they start to have some dysfunction and get remodelled until forming a very pathologic plexiform lesion that we can see in other types of pulmonary hypertension.
So this is a continuous process.
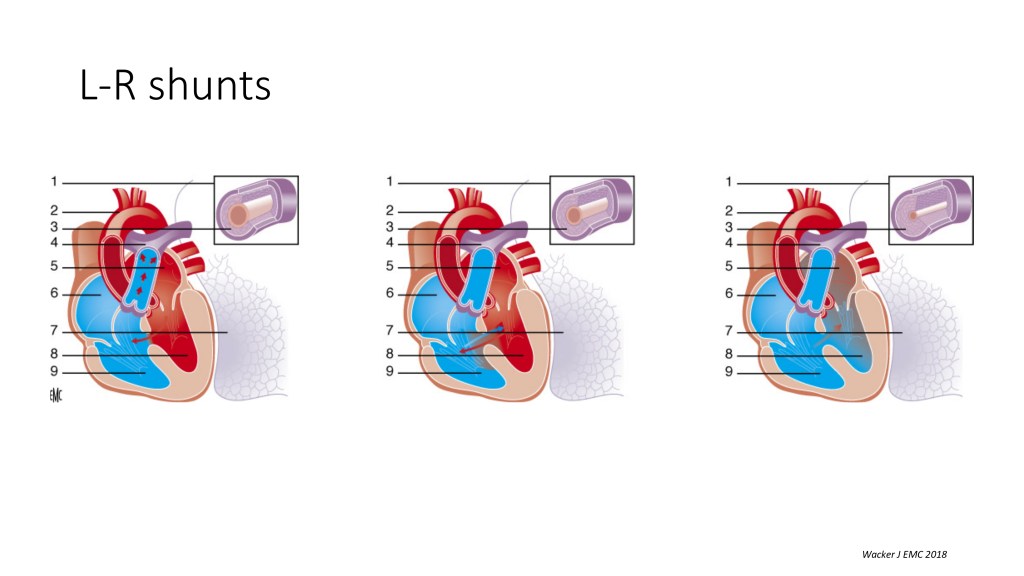
And when you have a left-to-right shunt, like let’s take a big ventricular septal defect, in the basal line situation, you have the shunt going from the left ventricle to the right ventricle and into the lungs, which increases the pulmonary blood flow. The arterioles are normal, but with the increased shunt, you have medial hypertrophy, and you have all the remodeling of all those little arteries in the lungs, and they get very sick. And at some point, the resistance increases so much that the shunt can reverse because the resistance in the lungs increases and is exceeding the resistance in the body. And that’s the end stage of a large left-to-right shunt that has not been treated before, and this is the Eisenmenger syndrome.
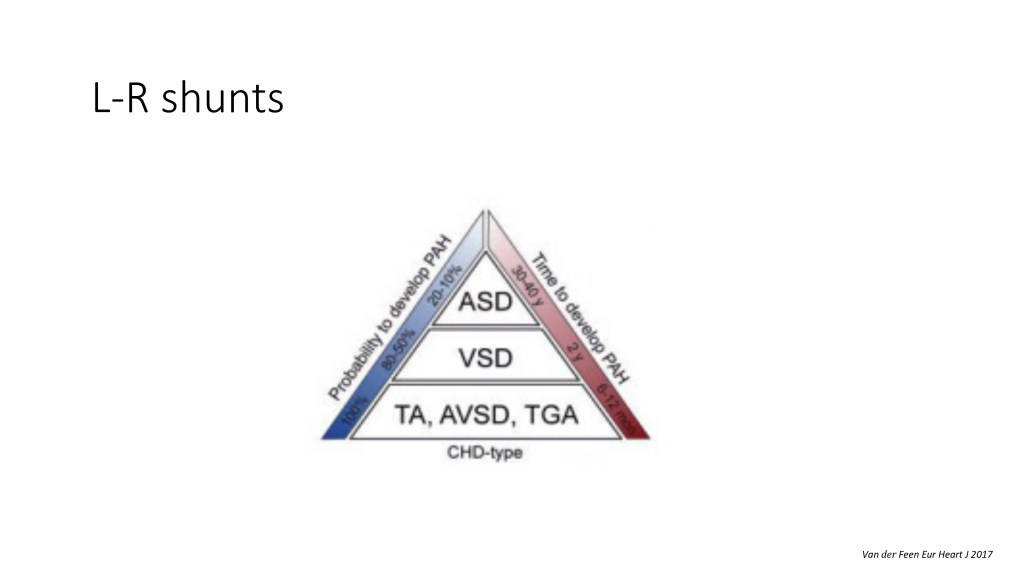
So depending on the type of your congenital heart disease, you can develop pulmonary hypertension sooner or, like, sorry, if you have a complex congenital heart disease with a shunt in the truncus arteriosus on AV canal, you have a high probability of developing pulmonary hypertension early in life. But if you have, like, a small atrial septal defect, you have very less probability to develop that pulmonary hypertension, and it happens much later in life.

And as I said before, it’s not, it’s a continuous process. So, you know, we know that with every left-to-right shunt, we have opportunity to close the shunt before getting to a zone of no return, when, after which, if you close the shunt, you can have persistent pulmonary hypertension because your pulmonary vascular disease is so advanced that it becomes irreversible. Or if you leave the shunt open, you can have Eisenmenger syndrome.
It’s very tricky to exactly know when you hit that zone of no return.

This is, I’m going to pass for the sake of time, but it’s the same, okay?
So, when you have a left-to-right shunt, you can have different situations.
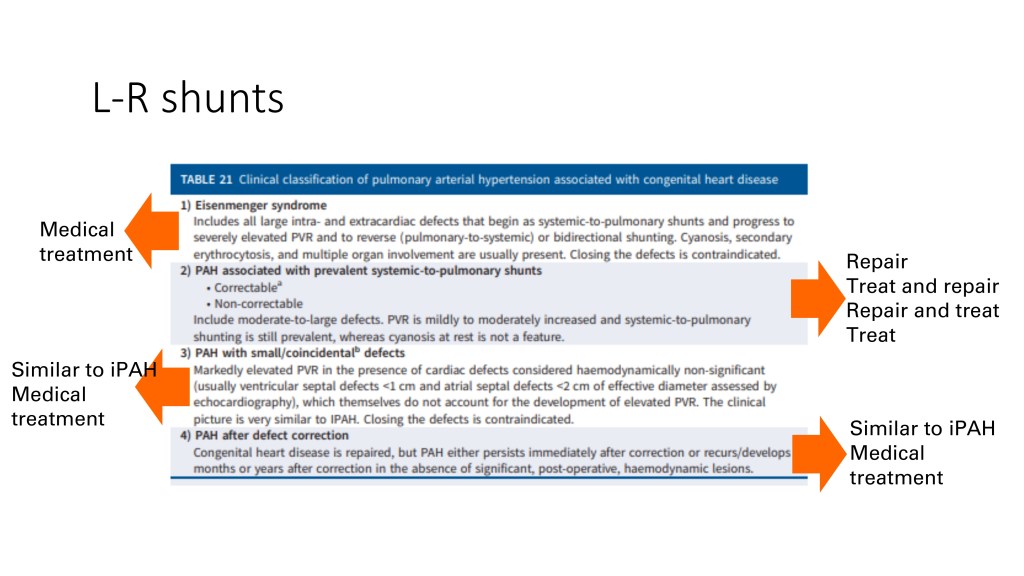
The most serious end of the spectrum is the Eisenmenger syndrome, where your pulmonary vascular disease is so important that your shunt has reversed, and for those patients, you shouldn’t close the shunt, but treat them medically. You can have pulmonary hypertension with a systemic to pulmonary shunt, not yet Eisenmenger. And in this group, you have to find which ones are correctable, and then you can close the shunt. And the ones that are not correctable because the pulmonary vascular disease is advanced, even though not Eisenmenger, you shouldn’t close the shunt.
And as I’ve highlighted before, we still need some evidence and some strong data to really know when a shunt is not closable. When you have a small defect, you have a pulmonary hypertension that is not believed to be caused by the shunt, and they are treated similarly to idiopathic pulmonary hypertension.
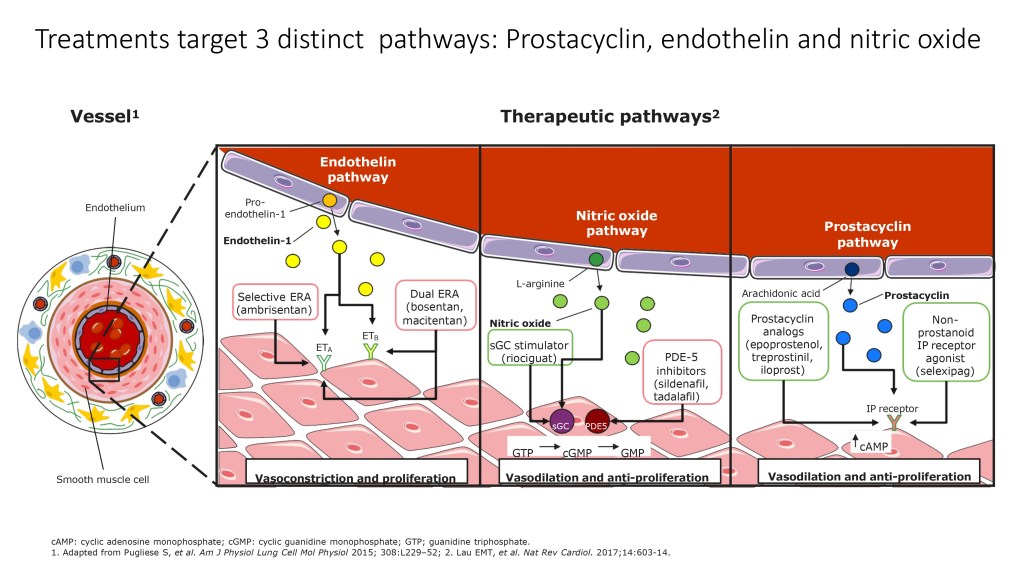
And pulmonary hypertension, after a defect correction that persists or recur, is also treated medically. I’m not going to go too much into details about the medical treatments that we use, but you know that they are targeting the three distinct pathways, endothelin, nitric oxide, and prostacyclin.
We’ve talked about left to right shunts and how they provoke pulmonary hypertension. What about left heart disease?

In left heart disease, you have this time, they belong to the Group II of the WHO classification, you can have acquired or congenital left-sided heart disease. And in that case, initially, you have the left atrial pressure that is increasing, that’s the main driver of the augmentation of the pulmonary artery pressure.
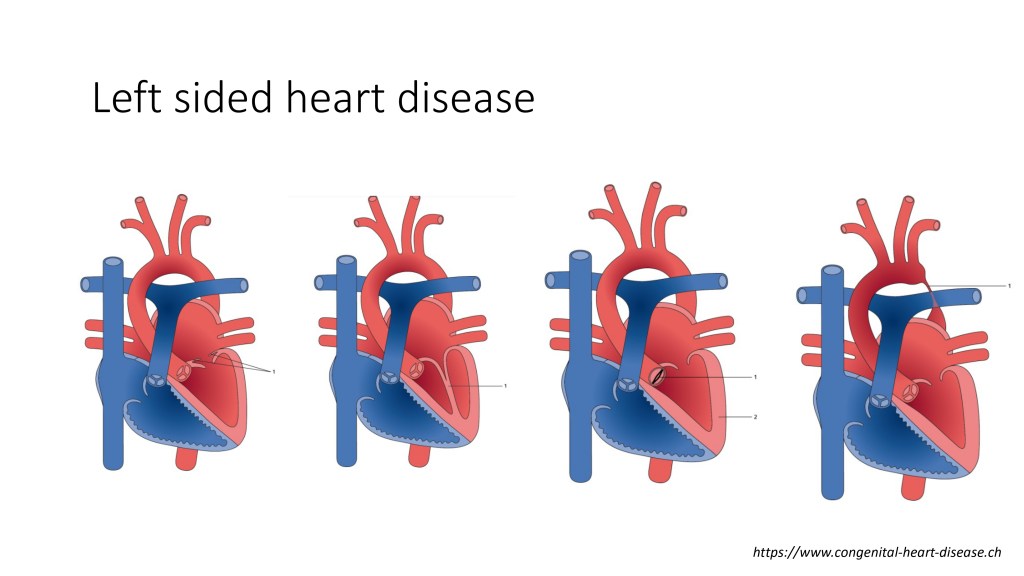
You can have a lot of different types of left-sided heart disease, a mitral valve anomaly, aortic valve anomaly, a coarctation of the aorta.
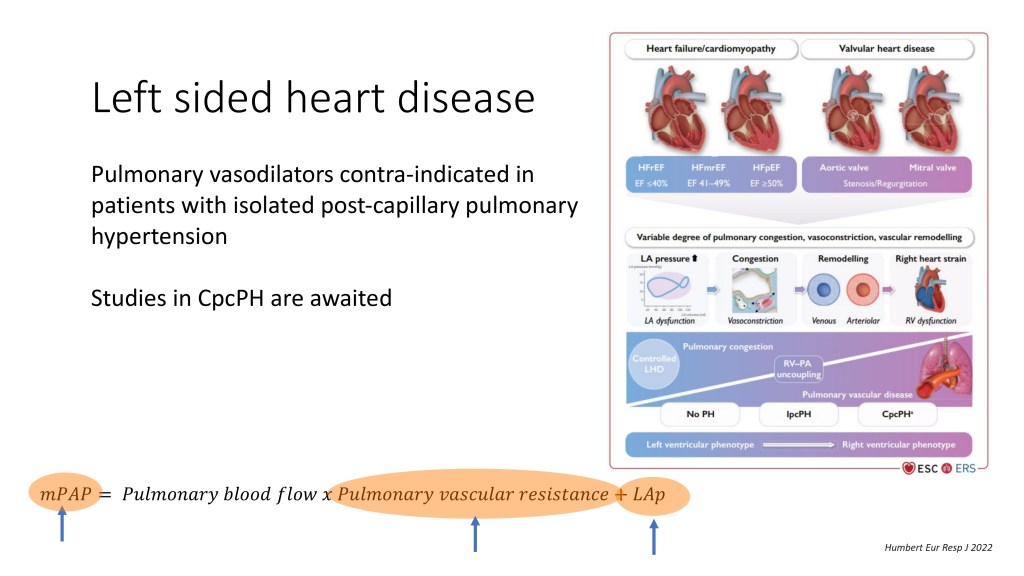
And in that left-sided heart disease group, when you only have this passive transmission of the postcapillary component, so the LA pressure to the pulmonary artery pressure, you shouldn’t treat them with a pulmonary vasodilator. However, there is a proportion of patients that, not only you have an increase in the LA pressure, but you can also have an increase of the pulmonary vascular resistance, because at some point, this postcapillary component provokes some changes in the pulmonary arteriole, and you have also a precapillary component that coexists with that.
And so the patients that have both postcapillary pressure that is increased, but also pulmonary vascular disease with increased pulmonary vascular resistance might benefit from the pulmonary vasodilators, but we still need to have some evidence for that.

The mixed mechanism, which is actually the congenital heart disease that is complex and which causes pulmonary hypertension by multiple factors and unclear etiologies are highlighted here. You can have segmental pulmonary hypertension, single ventricle, Scimitar syndrome.
I’ll come back to the single ventricle in a short while, but those are very complex congenital heart disease, they cause, or they can be associated with pulmonary hypertension, and we don’t have clear guidelines to guide our management.
And the last chapter that I wanted to talk briefly about today is the univentricular heart. So in a single ventricle, I’m just going to go slowly on this slide.
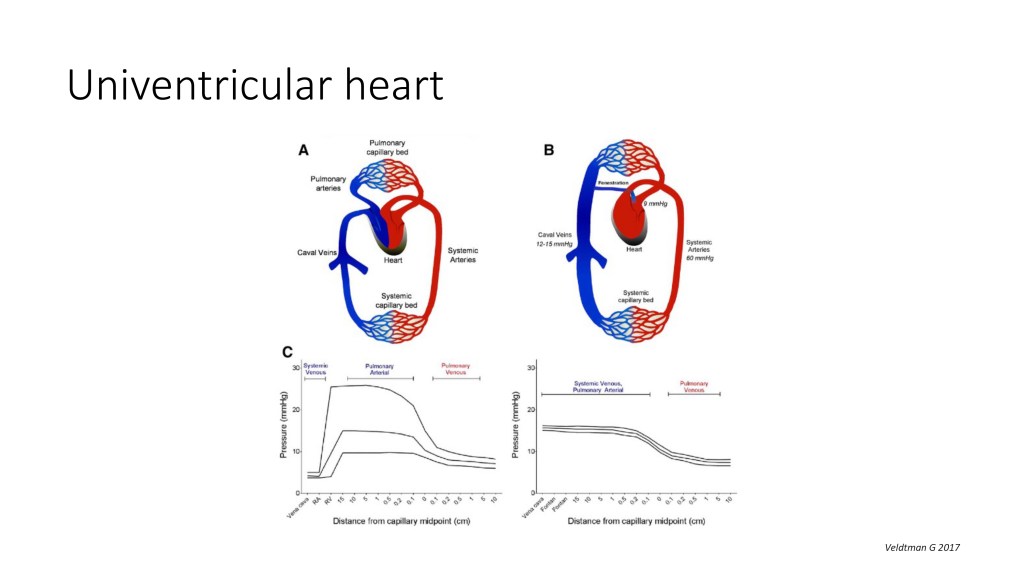
So in this drawing, you see a normal biventricular circulation. So you have your blood that is deoxygenated, comes back to the right side of the heart, is pumped into the pulmonary artery, gets oxygenated, comes back to the left atrium, and pumped by the left ventricle to deliver the oxygen into the blood and the body.
In a univentricular heart, which are patients that only have one single left or right functioning ventricle, they get all the series of surgery to get to what we call a Fontan physiology, which is actually the redirection of the systemic vein. So the systemic vein, they are plugged to the pulmonary arteries, so flow is flowing passively from the systemic vein into the lungs, coming back to the heart, and then the only pump that those patients have, the ventricle, pumps the oxygenated blood into the body. And you can see that for that physiology to work, you need to have a low pulmonary vascular resistance.
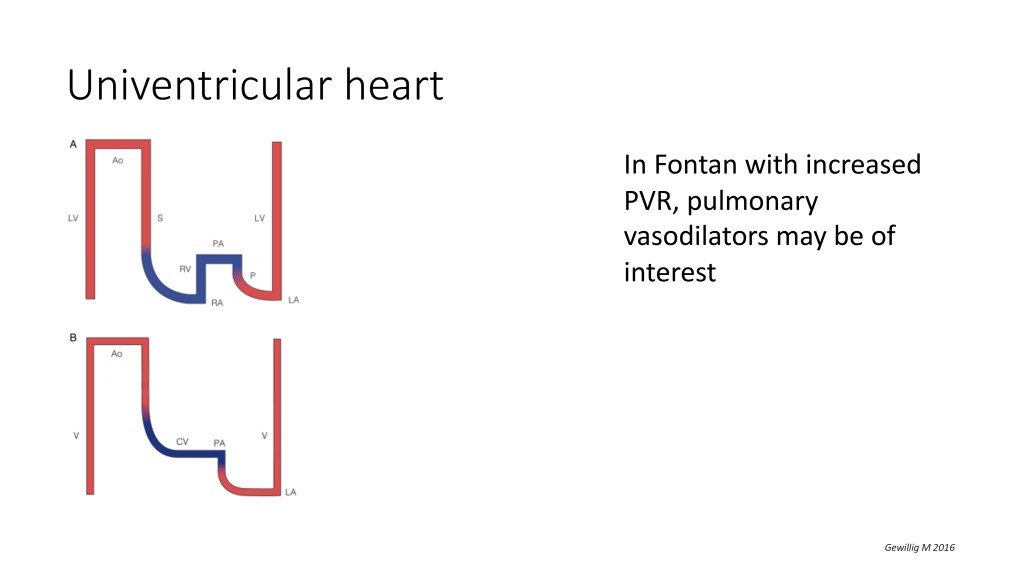
Those patients, they often don’t fit the definition of pulmonary hypertension, they don’t often have a mean pulmonary arterial pressure that’s above 25 or 20 millimeters of mercury, but they can have pulmonary vascular disease. And in those patients that have only one pump, and that have increased pulmonary vascular resistance, which needs to be demonstrated and calculated, those patients might benefit from pulmonary vasodilators. But again, we need more data from studies.
So to conclude, we still have a lot of work to do as a medical community, and maybe with the help of the parents associations and patients associations, we can help shape the future of research in pulmonary hypertension. But we really need to know if the pulmonary vasodilators can be of use in Fontan patient, if pulmonary vasodilators can be used in those left-sided heart disease that also have a combined pre-capillary component, or those that have a pulmonary vascular disease. And we need to better define the operability criteria in patients with an open shunt that comes a bit later than normal to see if we can close the shunt safely and if those patients can benefit in the longer term from a shunt closure.
So I hope this presentation was clear to you. I’m very happy to be here today, and I would be happy to answer any questions. Thank you.
ROBERT PLETICHA
Thank you very much, Dr. Wacker. That’s incredibly interesting and a good starting off point to now pass over to Professor Beghetti, and he’ll be talking about the transition from pediatric to adult care in pulmonary hypertension.
MAURICE BEGHETTI

Thank you, Rob. Hello, everybody. I’m Maurice Beghetti.
I’m also in the Pediatric Cardiology University Children’s Hospital of Geneva, and my task is to discuss transition. This is interesting because I’m quite an “old” person in pulmonary hypertension, and transition in pediatric pulmonary hypertension was not really something that was done many years ago because the outcome was not so good. But recently, I’ve been asked to discuss transition, and we will go through transition for congenital heart disease and pulmonary hypertension and show you what it means.
So what is transition? Try to define that.
Transition is the transfer from a pediatric clinic to an adult clinic. So transition is not just an event, but it should be a process, and I will insist on that over most of the slides. So what do we need?
We need physician understanding and education. We need patient education. Clearly, we need parents’ education because they were part of the problem for many, many years, and we need obvious hospital staff and administration education.
So it’s a healthcare priority. There is currently almost no real science behind this process.
It’s mostly, I would say, experience. There are few papers now that are coming into this literature, but it’s quite difficult to run a real study, and I think probably patient association will be very helpful in this process.
So congenital heart disease. So let’s start with that because it’s a mix today. We discuss a mix. Clearly, it’s a pioneer specialty in transition plans. There are well-established centers now that practice transition around the world. We have even, I would say, people that are trained in congenital heart disease in adults, and now transition is better.
We highlight the need for a team approach. I will insist on that. And the nurse is by far the most important person in this process because parents usually have access to the nurse, and they ask a lot of questions.
So we will discuss adult congenital heart disease, but we can discuss it with or without pulmonary hypertension. We’ll probably do a sort of combined approach in the next few slides.
We can see that in many pediatric diseases. All the chronic pediatric diseases are now planning transition clinics because congenital heart disease is one, but cystic fibrosis, cancer, sickle cell disease, all these different chronic diseases now need transition because we have made so much progress in pediatrics that these patients now are young adults, and they need to have adult care.
So, as I told you, survival is improving. And now the question is when and how to transition to avoid problems. And we have to remember that adolescence is a very vulnerable period.
Usually you reject your disease, and this is when you start to transition. So that’s quite difficult. And the problem, and we’ll discuss that, the main problem is loss of follow-up.
That means that they are not transitioned, they do not follow the transition, and they will not attend the adult clinic. And this is a big problem, more in congenital heart disease than in pulmonary hypertension.
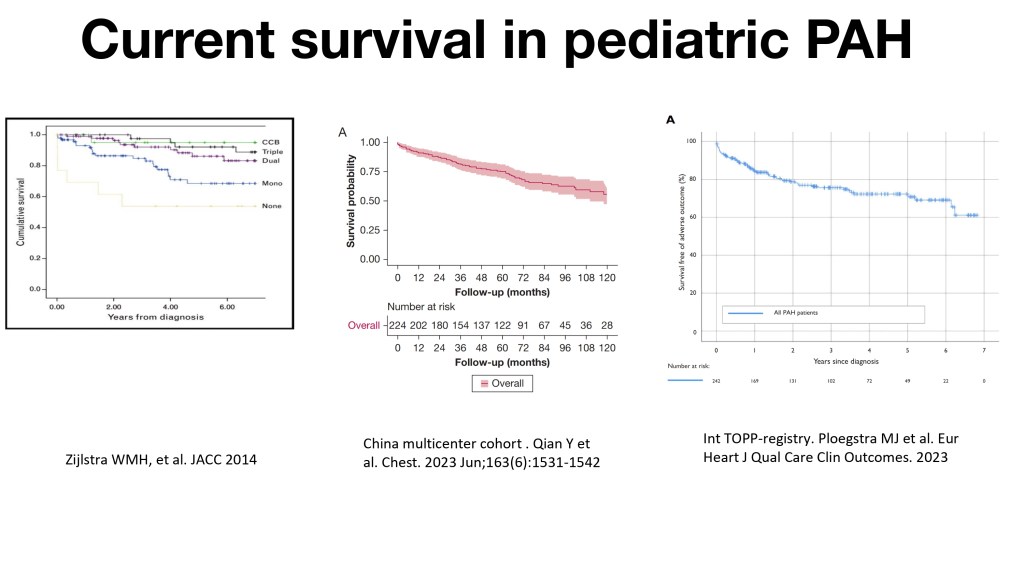
So, these are just three survival curves that explain why we need to transition. Compared to 50% survival at two years, we are now reaching, even if it’s not perfect, 60 to 80%, depending on the disease, of patients that may reach adulthood with this disease. And so they will need to attend an adult clinic because they cannot stay in pediatrics for all life, because we need to make space for new patients.
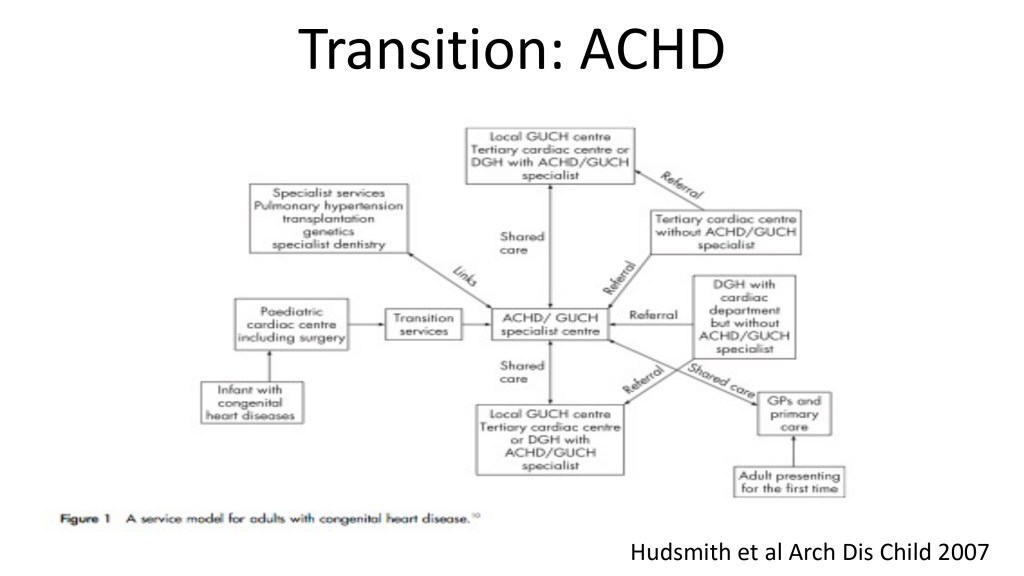
So, this is a complex slide, but you see that in the middle, you see the specialized center adult congenital heart disease called also grown-up congenital heart disease previously. And you see that there are links with different things. The link with pediatrics on the left, the link with outside hospitals, because sometimes it’s not always in the same hospital.
I will show you that we’re lucky in Geneva that pulmonary hypertension clinics are at the same place and congenital heart disease clinics are at the same place for adults and pediatrics. That’s very helpful, but it’s not always. And then you need a lot of specialty services around that, pulmonary hypertension for clarity, because we discussed pulmonary hypertension, congenital heart disease, but transplantation, genetics, dentistry, and all other organ specialists for this kind of patients.
So, you need to build a sort of program around your patients.

There is no gold standard, because I think every center is working differently. So, as you have your own practice, you need to build your own transition clinic adapted to your centers, pediatric and adult. For us, a bit easy, pediatric and adult clinics are in the same hospital. So, it’s very easy.
We have the same chart. We have charts that are transferred from one place to another very easily. And indeed, I’m running the adult and pediatric Pulmonary Hpertension clinic with my adult colleagues.
So, that’s quite easy, but it’s not always like that.

When is transition successful?
Is it when you send the patient to the adult clinic? The answer is definitely no. It is when the patient attends the adult clinic regularly. And that’s very important. If the patient is going only once, then you’re stuck, because you will lose your patient and you cannot follow him up.
So, why is transition difficult? I like this cartoon.
Patients are attached to their pediatrician. Sometimes we know the patients for 15, 16, 17, 18 years. And the pediatrician is also attached to his patients.
So, both feel very insecure about cutting the umbilical cord. And at some point say, okay, bye bye. So, it’s a very, very long gestation. And sometimes the transfer is not easy for everybody, patient, parents, and doctors.
So, why is it difficult? I told you, adolescence is a challenging period. Physically, because there are changes. Cognitive and psychological. So, you have to imagine adolescence may leave that with a lot of difficulties. For children with pulmonary hypertension, having a chronic disease, life-limiting, because they know that, there is more overprotection than there is even in congenital heart disease. And so, overprotection and insecurity by changing doctors is sometimes difficult. And there is indeed a difference. There is no science behind that, but it’s a feeling. It’s different if you diagnose a baby, and you follow the baby for 15 years, and then you transition the patient.
Then if you diagnose this during adolescence, during this very difficult period, and you rapidly transfer the patient to the adult. So, you have to take that into your mind when you prepare for the transition.

So, there are differences between adults and children. You will see some tables. I will not go into details, but you will have access to these tables when you have access to te recording on YouTube after.
Patient-centered care is the key in adults. The patient is dealing with themselves and the doctor. When you do that in pediatrics, it’s completely different.
There is the caregiver, the parents, other people, and this group needs to be transferred. So, in the adults, it’s more focused on the disease, and you discuss the disease with the patient. In pediatrics, you have to discuss the disease, the family, and the development of the pediatric patients.So, it’s a bit more difficult.
So, what helps success? I told you, proximity. The pediatrician should be proactive and support transition and not try to impede that. And adolescents will start to come alone at the pediatric clinics. It’s a bit difficult for pulmonary hypertension, but for congenital heart disease, sometimes between 16 and 18 years of age, they can start to come alone without the parents, and you can exchange and probably also discuss different things in the absence of the parents.
Prior to transition, assess and evaluate adolescent patient’s connective and psychosocial development, screen patients and caregivers for depression and other psychosocial problems, and prepare progressively for transition.
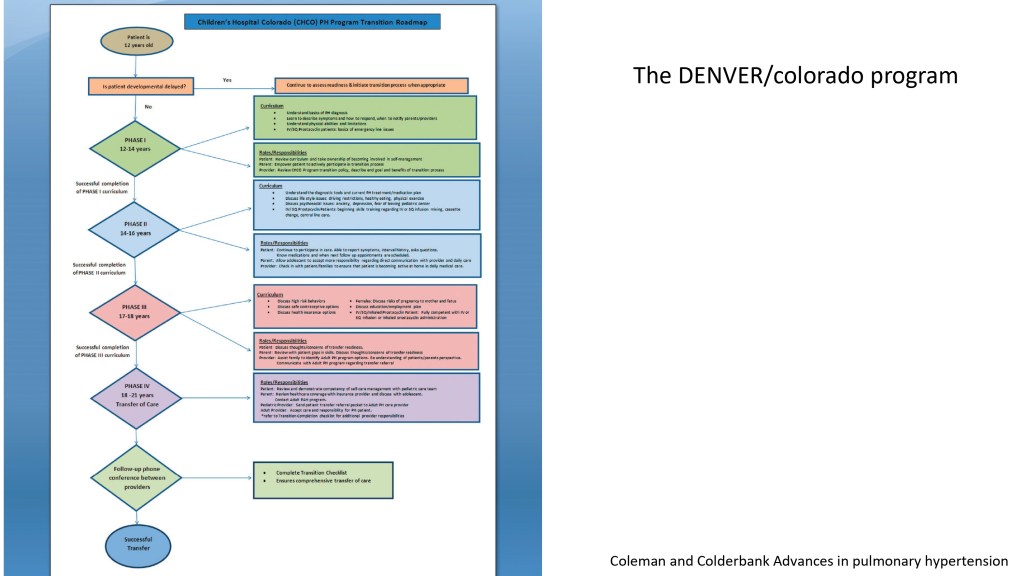
Usually, I start between 12 and 14. I discuss with patients and the family the adult concepts of care. I educate the caregivers, and I provide education materials if I have this available, and I review a lot of different goals with the family and the patients. For example, it’s not the same if the patient has a genetic disease or a developmental delay like a trisomy 21. All these things should be prepared, and usually 12 to 14 means that you start four to six years before you transition, because usually you transition at 18.

These are all the goals. I will not go through the goals, but there are a lot of different things: administration, medication, self-administration, prophylaxis for endocarditis, school, work plans, all these different things.
First, the last clinic visit before transition. So, you usually arrange the clinic in the pediatric clinic, but if you can, you should invite the adult doctor. And so, it’s a conjoined clinic, and the patient sees his future doctors, and he starts knowing. We review the medical summary. We discuss how the initial visit will be done. Sometimes you try to tour the adult clinic so the patient knows where he will go, and he will feel more secure when he will go there. So, he knows the new team, and we do that together.
Here is a checklist. I think it’s good if you can have access to that. That’s very helpful.
That’s a pulmonary hypertension checklist for pediatric patients going to adults. So, I will not go into detail, but it’s very helpful to check all these different things.
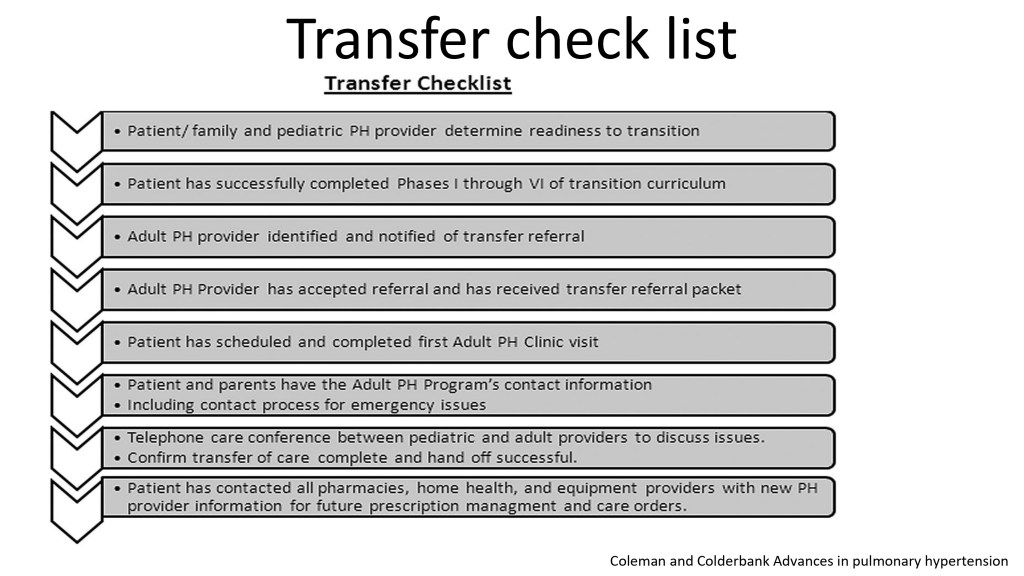
And you see, this is a summary. So, you see if it’s ready for transition, if he has passed all the different processes, if there is a pulmonary hypertension provider, adults, if there is a referral, if the chart has been sent, if he has access already to the phone numbers of the adult doctors, and all so on. And you check everything, and you check with the patient and the family if they have indeed done all these different things and are ready to be transferred.
So, the first adult clinic is a key. Sometimes I go to the first adult clinic, sometimes not.
But if we can do the same, it’s better. So, for the last clinic in pediatrics, the adult doctor is coming. For the first adult clinic, the pediatric doctor is coming. So, the patients feel that it’s just a follow-up. Nothing has changed. He’s secure and feels comfortable with the new team.
And we refine the role and the expectation for the patient, for the parents, and for the adult provider. And with this, the transition is a little bit smoother.
So, I conclude, and I conclude with everything as I have said during this. In a chronic disease, we must improve practice to be sure that you have no loss of follow-up. In congenital heart disease, there is a loss of follow-up. I think in pediatric pulmonary hypertension, with or without congenital heart disease, usually there is no loss of follow-up because there are a lot of drugs, treatments, and difficulties. So, usually it works quite well. But you need to really understand the factors that impact, indeed, the psychosocial approach of an adolescent and young adult to help him to transition as best as possible. And then the pulmonary hypertension therapies, they need to be adapted. We have, indeed, a sort of problem that is not a problem, but not all drugs are approved in pediatrics but are approved in adults so sometimes to switch can be a little bit complex, changing the dosage, things like that, clearly the two teams should work together so the patient will not feel that there is uncertainty about how to treat the patient.

I think that will be the last one, so a good transition needs a lot of effort and time, and never to underestimate the needs and the problems. You need to make continuous education of patients’, staff and administration. To stimulate the hospitals to do that. Chronic heart disease and pulmonary hypertension requires more attention due to dual disease and sometimes clinics. And I’m ready to answer questions if there are any questions.
ROBERT PLETICHA
Thank you very much Professor Beghetti. That was a very interesting topic that often goes neglected. To hear how you and your team are working there in Geneva, that seems very comprehensive, so now I’m going to pull up the slides of Kathleen, who is the mother of a young man living with pulmonary hypertension and she will tell their families story and journey, Kathleen over to you.
KATHLEEN
Hello,
I have been asked to share my story as a mother of a child with pulmonary arterial hypertension.
I am Katleen, I live in Belgium, and I am the proud mother of Vic. Vic has had pulmonary hypertension since he was 1.5 years old and is now 14 years old. He is a bon vivant, joyful boy with a tremendous amount of motivation and willpower.

His greatest passion is football and everything that has to do with darts. Our story has been different from most patients’ as we received the diagnosis before symptoms were clearly visible. Let me briefly explain how this happened.
Vic was born with a heart defect called “transposition of the great arteries,” which means that his two main arteries were incorrectly connected, preventing oxygen-rich blood from reaching his body.
Unlike pulmonary hypertension, this condition can be cured by open-heart surgery to correct the arteries, and life expectancy is good. There were some serious complications, but after five and a half weeks, Vic was able to leave the hospital in good condition.
Routine check-ups were necessary to ensure that everything remained properly connected. During a six-month checkup, an ultrasound revealed an enlargement of the right ventricle. A heart catheterization was needed for clarification.
I can still hear the cardiologist’s words: “Your son has a rare, serious disease called pulmonary hypertension … this time surgery is not an option.”

Many questions, fears and doubts followed. This was the beginning of an emotional roller coaster and our life with pulmonary hypertension. We knew nothing about pulmonary hypertension and through research and contact with the Belgian patient association we learned more about this disease.
The association still helps us with any questions we have. It’s a comfort to know that they will always be there for you. I recommend that you ask them what you want to know, rather than searching the Internet. But this can be scary for some, so take your time.
The feeling we had very quickly was: “We can’t take away his pulmonary hypertension, but we can do everything we can to give him the best life possible.
And that is how it happened.

Vic’s one of his first words was “ball,” so his passion for the game was evident at an early age. We knew his soccer career would be tough and short. But we didn’t hesitate to let him join a soccer club at the age of five. It quickly became clear that he was a natural talent who played the game with passion.
As the years went by, it became more and more physically demanding. He was forced to be in goal more often. At the age of eight, he made the brave but difficult decision to stop playing soccer.

We watched his last game with family and friends, with Vic scoring the last goal of the game and the end of his soccer career. There is no need to explain how emotional that moment was, but do we have any regrets about the fact that we let him play in a club? No! Because nobody can take those memories away from him or us.
Skiing was also something he really wanted to do. After consulting his doctor and receiving guidelines, we got the green light to go on this adventure. He couldn’t ski, and after trying one lesson, it became clear that his pulmonary hypertension. was limiting his ability to learn.
But that didn’t stop us from making the trip. We took the lift, Vic’s skis between mine, and skied down the mountain together. I am so happy we did it. What a beautiful moment.
Despite the many limitations, we always try to find a solution to do as many things as possible. Even if it seems impossible at first.
More limitations and more aids were needed as he got older. A modified stroller, then oxygen, then wheelchair, electric bike, etc.
Over the years, many adjustments have been necessary in school. Staying home when there were too many infections, taking a day of rest now and then, taking longer blocks of classes at home, to eventually a modified class schedule through homeschooling.
Your child is becoming more and more isolated, and as a working parent, you have to make sure he or she is taken care of. In my case, I am lucky enough to be able to work from home, although even that is not ideal. Vic is in high school and then you are supposed to go to school on your own. Where less carrying is needed for the parents, but for us it has only increased with the years.
So there are many additional things that come with it. A lot of people don’t realize this or don’t think about it.
Vic wanted a dog to accompany homeschooling. I didn’t say yes to it right away but in the end it was clear that this was the best decision. It is his faithful friend who makes him laugh or comforts him when he is going through hard times.
Since the summer of last year, his condition has rapidly decreased. As a result, he was recommended for maximum therapy. Starting Veletri pump medication.
Before that, he had been in a clinical trial for more than 1.5 years, this was his last hope to stabilize or improve his condition with medication pills but unfortunately with no result. It is likely that he was in the placebo group, which is the group that does not get the real drug. We had to stop the trial early. His therapy had to be increased to the maximum.
Due to the strict criteria which made it difficult to find suitable candidates, the study had a huge delay. As a result, the time for all patients to get the real drug was delayed until the end of 2024, which was too late for my son. Slap in the face and the hard reality of clinical trials.
The fact that there are less drugs available for children than for adults and clinical trial studies often start later for children, making treatment for children even more challenging.
One of our two biggest fears – “pump medication” – became a reality. One that has had an extremely significant impact on his life in the first place, and on our family also.
It turned out to be our last summer vacation without a lot of worries. Where he enjoyed the pool, the beach and jumping off high rocks into the water and so much more.
Beautiful memories made, but emotionally hard.
At the end of September last year, the pump was in use, and nothing is the same. His disease was already having a major impact on his quality of life, but with the pump, the impact is even bigger. Fear that his catheter will block, suddenly stopping his medication with potentially fatal consequences and so much more worries.
For the first few months, it felt like I was more of a caregiver than I was a mom. A lot of your time is spent on medication cassette preparation and providing care. You must think about so many things. For example, if you leave your house, you should always carry spare medication, spare pump and other medical supplies. When you go on vacation, you need to know where there is a hospital in that country that treats pulmonary hypertension, because only they have the expertise.
It also has a lot of side effects that can cause a lot of pain and discomfort. With Vic, these side effects are strongly present. You live every minute with a line coming from your chest, always connected to a pump.
So many limitations for a child who should have been in the prime of life. I find this so hard for my son and all the other children with this disease.
Against all odds, the pump medication is not working for my son. His condition is still rapidly worsening, so we are already in the next stage of the process which is the development of his transplant plan. Our biggest fear.
As a parent, it is incredibly hard to watch your child become sicker and more isolated because of his or her illness. They are constantly in a battle, both physically and mentally, against the limitations of pulmonary hypertension. From a young age, they have to consider what they do and don’t do. Facing the fact that other children are doing what they want to do with a lot of energy. Even as a parent is this confronting because you are so powerless.

What does help us a family is to always have a good laugh even on the silliest things and to keep communicating openly.
We decided from the beginning to be honest with Vic about his illness, no matter how hard the answer was. It’s his body and his life, not ours. Trust is the most important thing for us.
Here, taking oxygen is the biggest discussion point. Where we as parents want him to take it in more often. He also knows that this is important to him. But it is often too much for him. We then try to come to an agreement around that, rather than just saying you’re going to do this now.
I always thank him when he takes oxygen because I don’t take it for granted. We had many emotional conversations I never thought I would have to have with my child. He knows that we will answer every question very honestly, so he has full trust in us.
Chronic mourning, mourning for a loss that never ends, is faced by every pulmonary hypertension patient or parent of a patient. You constantly have to adapt to significant changes in your life. People around you expect that once you are confronted with this pulmonary hypertension problem, you quickly process it, give it a place.
You accept your child, but not the limitation it has to live with every day.
You often face cruel, thoughtless, and harsh comments or do not receive the support you hoped for. Unfortunately, also from closer friends or family.
But also new friendships have been made. Surround yourself only with people who give you energy, listen to you, and are there for you.
The work-life balance is quite intense. I have a full-time job that I have to combine with the extra care, which is quite difficult. After starting the pump medication, I stayed home for four months, then returned to work part-time, and now work 75%. My job is my distraction, it is the only place where the future is not my biggest enemy.
What is important in my opinion?
Let your child do what he or she wants to do, despite your own fears. Just be there if they did do much and need your care.
Try not to say, “See, I told you it wasn’t a good idea,” Not really the answer that you want to hear from somebody else at that point. It’s easier said than done, I know that from my own experience.
Talk openly and honestly with your child, but above all, listen to your child. Let them also decide when they want to proceed and how they want to do it. Give your child as a teenager a voice in their treatment – it’s their life and body.
As parents, we have a different way of thinking because we want our child to be with us for as long as possible.
I keep reminding myself how I was as a teenager and what my priorities were. How would I have reacted as a teenager? It’s not easy to deal with as a mother but still much easier than living with pulmonary hypertension.
Be an advocate for them in difficult conversations with their doctors and fight for their quality of life. Doctors, unfortunately, often think only about the medical aspect and not about the impact on the patient’s life and that of the family.
Do not postpone – life is now, later it may be too late.
As a parent, don’t be too hard on yourself, give yourself a break as well. If you or your child are having a bad day, let your child stay home from school for example and enjoy the time together. A day like that is going to give you a lot of energy.
And most of all have a good laugh and have fun! Make memories!
Thank you for listening.
ROBERT PLETICHA
Absolutely wonderful advice Kathleen, and i want to thank you and your whole family for sharing, sorry that Vic had to grow up so fast and already faced adult issues and you guys are doing the best you can and you gave us advice about life in general, i want to share a few comments. “Lots of love to you Kathleen” and Louise Bouman said that “It’s good to see that Vic can try so many things he enjoys, very important and so nice to see him with his dog. I have tremendous admiration for you as a parent”.
Pisana Ferrari from Alliance for Pulmonary Hypertension says that its a very inspiring presentation and thank you Kathleen for sharing. Nadia thanks you as well. We have some questions about the medical side.
For you Professor Beghetti we have a question for you from Louise, she heard that the most difficult thing about transition is both for the patient and the parents, the patient is all of the sudden in charge and the parents are on the sidelines and its for both pretty difficult. How could they both be prepared for this transition?
MAURICE BEGHETTI
I think this is what I tried to explain previously. You have to be both prepared in advance. I fully understand because the parents are being involved for a long time and the testimony of Kathleen explains it, I mean you are involved as a mother and when they become adults you are still there, so sometimes it’s difficult to give some space also to the patient, it depends a little bit but this is the theme to involve the parents as much as possible but also to give the patient the chance to start to take care of himself because if this lasts for a long time he also needs to live by himself in some ways depending on the degree of the disease and you need indeed to do this but the parents as i told you and you have seen the picture of Kathleen. You have an umbilical cord as when you have a child that has had such a difficult disease for so many years it will be a bit difficult.
So physicians and nurses, psychologists, psychiatrists sometimes all need to be involved since very early in the disease not only when things go wrong. It should be from the very beginning. The teen should be prepared for that and the doctor should be very experienced in this disease to organize that in some ways. If the doctor is very confident and knows the treatment very well, it will be easier. But I saw some cases where the parents want to be there in the magnetic resonance imaging suit and computed tomography scan suit and the adults feel it’s a little bit difficult unless there is some kind of developmental delay such as trisomy 21 or a serious problem. But that’s the point when you need to make the change progressively. You are still involved but you have to smoothly make the change then I would have too many comments on what Kathleen said but they will probably be too many: the trials, the drugs, the transplants, the disease. How to explain that. I mean Kathleen’s boy has a rare among a rare disease because transposition of great arteries with pulmonary hypertension is extremely rare and of course it’s so much different from other types of pulmonary hypertension this is difficult but i’m working on giving drugs earlier better than later and I think the authorities started to understand that families don’t like placebo controlled trials.
ROBERT PLETICHA
Yes especially in a rare disease where time is quite so important.
Here is a question for either Dr. Wacker or Prof. Beghetti: Does your center provide psychological support for parents or children.
JULIA WACKER
Yes we do, all our patients with chronic disease have some sort of psychological support. It’s always proposed but it’s not always taken and it’s important to re-offer depending on the situation, because it’s always a step for patients and parents to accept that help. I think if there is an opposition or not wanting to take this support I think things change and it’s a duty for us to really offer.
MAURICE BEGHETTI
They must have this support but the problem is what is the type of this support so it depends on the size of your clinic. If you have a big clinic with so many patients you may have a special psychologist that is in your team and that’s easier but if but if you are a small clinic then its difficult and the hospital will offer you a single person dealing with that so the adults definitely have that, the pediatrics clinic they have a psychologist in their clinic and they know how to approach parents and how to help them then we have a specialized psychologist for the pre transplant programs and that’s also a different step.
ROBERT PLETICHA
If your center is in contact with pulmonary hypertension patients associations?
MAURICE BEGHETTI
Switzerland is a strange country because we have so many languages. We had a pulmonary hypertension french-speaking patient association but it’s over because you need people running that and usually they are patients or parents or something like that.
But in Germany there is one, but we are linked to the French one. Every year or twice a year there are meetings for parents and patients association and thats french-speaking so we are more linked to this part and then we are linked with the USA association where we had parents association in decisions of treatment trials So yes, we are linked maybe not as much as we wish but we are a small part of Switzerland.
ROBERT PLETICHA
And Kathleen, I want to give the last comment to put you on the spot here. Did you have any question or comment for the many things you heard from dr Wacker or dr beghetti.
KATHLEEN
Well maybe about the transition and that is something that I’m going through already, as you saw I know Vic’s doctors since he was born, after we moved to the study we moved to the adult department, it was a big difference for us and its something that I’m worried about as well but I try as much as possible to inform vic about it but its its something interesting that I’m worried about because you will always stay a parent and that will never change but he needs to have his own life and we try already. For example if Vic says that he wants to stop the pump medication then we will follow even if we as parents we don’t want to but we have to follow his wishes.
ROBRT PLETICHA
Yes it’s true.
MAURICE BEGHETTI
How old is Vic?
KATHLEEN
He is 14
MAURICE BEGHETTI
Well it’s not time to discuss that but I’m sure your center or others will come with other possibilities. Since your son is very strong, there will definitely be other solutions.
ROBERT PLETICHA
Thank you all for the very nice webinar, we enjoyed it a lot and to our speakers thank you very much for coming and speaking and to our audience the next webinar will be on the 18th of June and its about genetics in pulmonary hypertension so we look forward to seeing you back here at that point and in the meantime check out the pulmonary hypertension knowledge sharing platform for this and other webinars and tons of great resources.
Thank you everyone and wish you a great day .