
When science and AI converge: the evolving landscape of Pulmonary Arterial Hypertension (PAH) care
Organized by the Alliance for Pulmonary Hypertension
Dr. Andreas Reimann:
Welcome to this first webinar in a series of four webinars organized by the Alliance for Pulmonary Hypertension this year. I am very happy to welcome you on this Friday evening, and I appreciate you taking the time to join us for a very interesting topic: “When science and AI converge: the evolving landscape of PAH care.”
I am Andreas Reimann, and I am a co-founder of the Partners4Patients Foundation. We have supported the Alliance for PH as its Secretariat for the last four years, and we are proud to work with such a talented and dedicated team. I am also very honored to be joined today by four excellent speakers who will share their experience and insights with us.
Please write any questions you may have in the chat at any time, and we will try to address them during the final part of today’s webinar. The webinar is planned to last about one hour.
Without further ado, I would like to introduce our first presenter, Professor Lis Neubeck from Edinburgh Napier University, who will speak about digital health and its potential to improve patient care.
Prof. Lis Neubeck:
Many thanks. I hope I have my slides up as well. Thank you so much for the invitation to speak today.
What I want to cover is a brief summary of what we know about digital interventions and why I became interested in digital tools. My background is actually as a cardiac rehabilitation nurse, and I was interested in this area because not everybody gets access to cardiac rehabilitation. We know that many cardiovascular events are repeat events, and we know that going to cardiac rehabilitation improves cardiovascular risk factors and quality of life and decreases morbidity and mortality. But cardiac rehabilitation, as it exists for those of you who have been able to access it, is typically time-limited, facility-based, and conducted in groups. So I became interested in how mobile apps, social media, and wearable sensors might increase access to effective prevention.
Thinking about digital health in general, the terms are often used interchangeably, and the strict definition is a little woolly. But in terms of what I am talking about here, I mean telemedicine and remote monitoring, the use of AI and big data, wearables and mobile health, and electronic health records.
When we think about cardiovascular disease prevention—and forgive me for leaning toward that, because I realize the interest here is similar, but not identical—we have the opportunity to use wearable devices to support self-management. This is something that is increasingly useful. Another helpful point is that if you had a wearable device before your initial diagnosis, you may already have a benchmark. You know where you were before, and that can help us predict and plan from there in terms of what you want to achieve.
There are huge numbers of mobile apps for lifestyle modification. Some of them have been explored very well in clinical trials; others are created very quickly and are not necessarily the most robust types of interventions. There is also huge attrition in mobile-app use, which is problematic when we consider their long-term value.
We are also beginning to see the emergence of AI risk-prediction models. That may be beneficial because we could potentially detect disease before it emerges in its clinical stages and ideally prevent some of the problems that result from it. We can also use digital technology in diagnosis. We are now at a stage where we can look at ECGs years before disease emerges and make predictions. Echocardiography interpretation is also now being done in an AI-assisted way. And we know that AI, if it is appropriately trained and the models are right, can actually be better at detecting some particular facets of a condition.
However, this is the important point: AI still creates what we call hallucinations. It sometimes makes things up because, effectively, there is a numerical model behind all this, and it is predicting based on number patterns. So it does sometimes make things up, but it can also help us manage large amounts of data.
In terms of diagnosis, we know that remote blood pressure monitoring and cholesterol monitoring are hugely successful ways not only of detecting problems but also of treating them effectively. We have just run a large project in Scotland looking at providing people with blood pressure monitors, and we showed that over time—and particularly during COVID—there were significantly fewer cardiovascular events in the group that got remote telemonitoring compared with the group that did not, even though they were otherwise managed in the same way. And, of course, we can use machine learning for early detection of arrhythmias, and we can predict atrial fibrillation based on an ECG taken something like five years in advance.
So these are really exciting times for us.
We can use digital health to support and manage conditions. We can have telemedicine for follow-ups, and we can use it to remind people to take medications. When you think about taking medications, particularly some of the medications used for preventive health, you need both the capability to take your medication—you need the prospective memory to plan and take it—and also the understanding of why you should take it. Digital tools can potentially help with that.
We also have a number of implantable devices that provide remote monitoring, and this is particularly important for detecting heart failure, for example. And we can use AI to help drive decision support for clinicians. There are some interesting papers suggesting that AI is more empathetic than clinicians. I think that says more about us than about AI, and that we need to be a little more mindful of how we interact with patients.
The core components of digital health matter. It needs to be persuasive. It needs to employ convincing and effective communication. We know that people change behavior only when they have sufficient motivation, ability, and appropriate triggers. Behavior change is most likely to happen when an app is widely used by consumers and when a number of core components and ideal features are present. These are things we can use to determine whether an app might be effective.
I am just going to give you a couple of cases where this might be something we could consider. For example, in atrial fibrillation, we know that we can detect it from smartwatches and wearables. The biggest study to date is the Apple Watch Study, but one of the challenges around that study is that although they screened a very large number of people, they screened a relatively young population who were not that likely to have the disease. So, we are really creating a tsunami of data with relatively little effective management.
Photoplethysmography is available; it works in a similar way to oxygen-saturation monitoring and can detect changes in blood flow that may pick up abnormal rhythms. We now know that atrial fibrillation may be detectable through cameras on iPhones, and there is emerging work suggesting that voice changes may also be informative. Blood pressure monitors can also be adapted so that they detect atrial fibrillation. So digital technology can support early diagnosis and perhaps make achieving a diagnosis more accessible.
Just by way of interest, there is a paper by Emma Svennberg and colleagues on how to use digital devices to detect and manage arrhythmias. They discuss whether people are ready for this technology, how to select the right type of technology, how to provide education, how to assess support needs for using digital technology, and how to agree on a health-monitoring plan. I think that as we all age, it will become less and less complex for us to use digital technology. We still have people who are not used to it, but we will get to the stage where everybody is.
In heart failure, we can use digital tools for teleconsultation, so we can provide remote care. We can use digital scales that report changes in weight; in heart failure, a sudden change in weight may indicate fluid overload. Again, we can use wearables. We can also monitor thoracic impedance to see whether there is congestion. And we can provide remote rehabilitation—for example, teleyoga has been successfully tested in a population with heart failure.
With implantable devices, we can also do remote haemodynamic monitoring. The challenge with all of this is making sure that there is somebody there to provide the clinical care if there is a need to act on the monitoring.
For me, the benefits of digital health are that it can provide equitable access to care, support early detection and intervention, improve patient engagement, and enable clinicians and patients to work more closely together. Of course, it may also reduce healthcare costs, particularly when you take into account indirect costs such as time off work and travel to appointments.
There are, of course, challenges and barriers. I mentioned the amount of data that comes from these devices. We have a tsunami of data and patients seeking confirmation of diagnosis. How do we address this? It may also shift our focus and make healthcare more reactive rather than proactive, because all we are doing is dealing with data. We also have questions about how we keep the data, how we store it, how we interpret it, and who owns it. My argument would be that the patient should own it, but of course that is not always the case, and data is valuable to big corporations. So we need to be mindful of ethics and data privacy when we consider digital options.
My final recommendations would be to adopt a patient-centered approach to digital tools, ensure digital inclusion—so do not expect patients to pay for this themselves—invest in AI-powered decision support, make sure the models we use are robust and tested in different populations, strengthen data protection, and collaborate across healthcare, technology, academia, and, of course, with patients to make sure what we provide is truly appropriate for the individuals we want to serve.
Dr. Andreas Reimann:
Thanks very much, Lis, for this very insightful presentation. I think it was a great start to this webinar. And indeed, to the audience: please use the chat to key in your questions, and we will address them at the end of the session.
I am now very happy to welcome our next presenter, Wendy Gin-Sing, who is a Pulmonary Hypertension Nurse Consultant at Hammersmith Hospital, Imperial College NHS Trust. Wendy, over to you.
Wendy Gin-Sing:
Thank you. Like Lis, I also have a background in cardiology—over 17 years in coronary care—but I have been working in pulmonary hypertension for about the last 26 years, so I have seen quite a lot of changes over that time.
I am going to talk more about the teleconsultations that we have in the pulmonary hypertension service and what we can do for follow-up. In the UK, we have six designated specialist centres, and those were all set up about 26 years ago. As you can see, they are not evenly spaced across the country, so many of our patients have five or six hours of travel to get to our pulmonary hypertension centres. I know that in some countries that is considered quite a short distance, but certainly when you live in the UK, that is a long time out of your day just to get to an appointment.
Remote consultations were prompted by our patients living a long distance away, and then were really accelerated during COVID because patients could not travel to the specialist centres. All the red tape and difficulties we had in setting up video consultations around security and data management suddenly melted away, and we were able to use a variety of platforms to speak to our patients via video. They were able to access these on their phones, tablets, or computers.
What really surprised us was that a lot of the older population, who perhaps had not used much technology before, learned during COVID to use Zoom and many other ways of communicating. Another positive aspect was that several people could be in the virtual room at the same time with the patient. That might include the local consultant, the consultant from the pulmonary hypertension centre, nurses, the patient, and sometimes relatives who were not actually in the room with them.
Being able to see somebody on the screen improves communication. When you are looking them in the face, you can see how the information is landing, whether they are understanding it, and whether they are agreeing to it. That is incredibly important when you are discussing quite complex drug therapies or diagnosis, and certainly prognosis and emotional subjects as well.
We also found it really useful for troubleshooting problems. When pumps are alarming or there is a problem with a line, it is much easier to sort out if you can actually see it over video than if somebody is trying to explain it over the telephone. Likewise, if somebody has fluid retention and oedema, it is much easier to be able to look at their legs and see how swollen they are.
That said, the majority of our remote consultations are still by telephone. This is preferred by a minority of patients who cannot manage the technology for video, and many people prefer it simply because it is easier.
When we started doing lots of remote telephone or video consultations, we found that many of our patients were not approaching them in the same way as they would if they were coming to hospital. Sometimes we would be trying to talk to somebody and they had gone out shopping. I have had two conversations with patients in the drive-through at McDonald’s while they were trying to place their order. So we worked with the patient association to try to help people make the most of remote appointments.
They produced an information leaflet, and really it gives patients time to think about what they want to discuss, how well everything has been working, any new symptoms they have, and to make a list of their medications—so really to be prepared for the appointment in the same way they would be if they were coming to hospital, perhaps even a bit more because it is remote.
In our remote clinics, it was really important that we got the same kind of information remotely that we used to get in person. Patients would do six-minute walk tests at home, and there are now many apps that can support six-minute walk testing. The most popular one we found was Strava. Patients would time their walks, and most of them would have pulse oximeters so they could see what their saturations were like before and after the walk. They would then send us the information from Strava.
We also sent them blood boxes so they could get their bloods taken locally and sent in to our centre, so that we could analyze the results and discuss them when they were in clinic. And as Lis mentioned, there are devices that can send through a patient’s weight, blood pressure, heart rate, and oxygen saturations. A small number of patients also have handheld cardiac monitors that allow them to check their rhythm, and more of them now have watches that can pick up abnormal rhythms.
We also get their average daily step count. That is really interesting, because some patients, when you ask them about their activity, say, “Oh, I am very busy all day. I am always on my feet and I do lots,” and then you find they may only do 2,000 steps. Other people say, “I really do not do as much as I should, and I really ought to do more,” but they are actually doing 7,000 or 8,000 steps. We can also monitor actigraphy, so we can see exactly what they are doing.
When we have collected this information remotely, we are able to risk-score our patients. This is a mortality-risk assessment and helps us judge prognosis and whether we need to change therapies. We use this risk score to inform decisions about drug escalation. What we really want is for all our patients to be in the low-risk group, in green—functional class I or II, walking a long distance, and with a low BNP. By sending in that information, we can make a clinical assessment of how well they are doing.
But we also like to have even more information, and we have already mentioned some of the implantables and wearables. The one we are using more and more in pulmonary hypertension is the implantable CardioMEMS device. It is inserted during right-heart catheterization; it is a very small device that sits inside the pulmonary artery and stays there lifelong.
At home, the patient lies on a small pillow after resting for 10 minutes, presses a button, and then sends the information through. That gets saved every day, and we can access trends and see what their pressures are doing. When they come to hospital, we have additional equipment that can talk to the CardioMEMS, and we can find out what the cardiac output is—so how well the heart is really working.
A lot of patients are getting small implantable ECG monitors that go under the skin in the chest. They then sleep next to a little box, and the two devices talk to each other. Their heart rhythm is sent into a central database, and we get alerted if they have abnormal rhythms. We have also spoken about actigraphy monitors, and I will show you a picture of the kind of information we get in a minute.
Step counters are really very interesting, especially when talking about rehabilitation, because then we try to get patients to increase their steps in small increments. This is the kind of information that we get from actigraphy. It is colour-coded. The dark blue at the bottom is the amount of time spent sedentary. The red is light intensity, and moderate intensity is the light blue. If you have patients who do vigorous activity, such as going to the gym or cycling, that will show up as well. It gives a nice overview. Over several months of data, it may show that patients are fairly stable, but every now and again they will have a day when they really do not do very much because they are feeling unwell and perhaps do not get out of bed. So a six-minute walk tells us what you are like at one moment in time, but actigraphy tells us what you have been up to more broadly.
Another way we use technology is through a cloud-based platform that supports our patients who are going onto selexipag and some of our other more complex therapies. We are able to send them information via an app on their phone. Each week, before their telephone consultation about titration, we send them a questionnaire. They fill it in and tell us about the side effects they have had, how severe they are, and what drugs they have used to manage them. Then, when we speak to them on the phone, they have had time to reflect on the last week, and we already know the areas we need to address.
While we are collecting all this medical information, it is also really important to collect quality-of-life data. We send our patients remote quality-of-life forms to fill in, and that is essential because it can pick up psychosocial issues that will not necessarily come across on a six-minute walk test or an oxygen level. Our patient association also has several resources for people at home, including self-workbooks for anxiety and depression, and they run a listening line. It is really important not to forget quality of life and focus only on the pressures.
So, just to conclude: remote follow-up to decrease the frequency of visits is certainly feasible, and I think it is going to become even easier with more technology. It means we can keep a very close eye on people who live a long distance away and monitor them between visits. But there is still a need for visits to the pulmonary hypertension centre. In the UK, it is mandatory that all patients on therapy have at least one face-to-face visit every year, just so that we can see them and address any other problems.
Dr. Andreas Reimann:
Thank you. Thanks very much, Wendy, for this very comprehensive talk. It is fascinating how you managed to cover this big subject of teleconsultations in PH care within 10 minutes. Thanks so much for keeping to time and for being so comprehensive. Once again, please use the chat to send in your questions.
I am now very happy to welcome a patient testimonial from Hall Skåra, founder of PHA Norway and project manager within PHA Europe. He is going to talk about home monitoring devices and wearables from the patient perspective. Hall does not seem to be able to join us properly at this moment in time. Dr. Ghofrani—perhaps we go ahead with your presentation. Apparently Hall has some difficulties. If you do not mind, then please go ahead.
I am very honored to welcome Professor Ghofrani, a renowned PH expert, Medical Director of Universitätsklinikum Gießen und Marburg GmbH and Director of Research at the Kerckhoff-Klinik. You are going to talk about innovations in drug delivery to improve the patient experience. Professor Ghofrani, please.
Prof. Ardeschir Ghofrani:
Thank you, Andreas. Thank you to Pisana, and thank you to the PH Alliance for organizing this meeting.
I am very happy to share our thoughts on innovations in drug delivery to improve patient experience, because I think we all agree—and I particularly hope our patients agree—that drugs should not only be efficacious, but should also be comfortable to use and well tolerated, which in turn increases patient satisfaction with treatment.
Let us remind ourselves that the field of pulmonary arterial hypertension has seen rapid progress over the past two decades. We started in the late 1990s with virtually no options available, and then came an extraordinary and unprecedented expansion of pharmaceuticals from different drug classes and different routes of administration. This has transformed pulmonary arterial hypertension from a frequently progressive and unfortunately often deadly disease into one that is, many times, very well controllable nowadays.
But for established treatments, as well as for some of the newer upcoming treatments, considerations around side-effect profiles—and the route of administration, which is often related to undesirable adverse events—remain crucial.
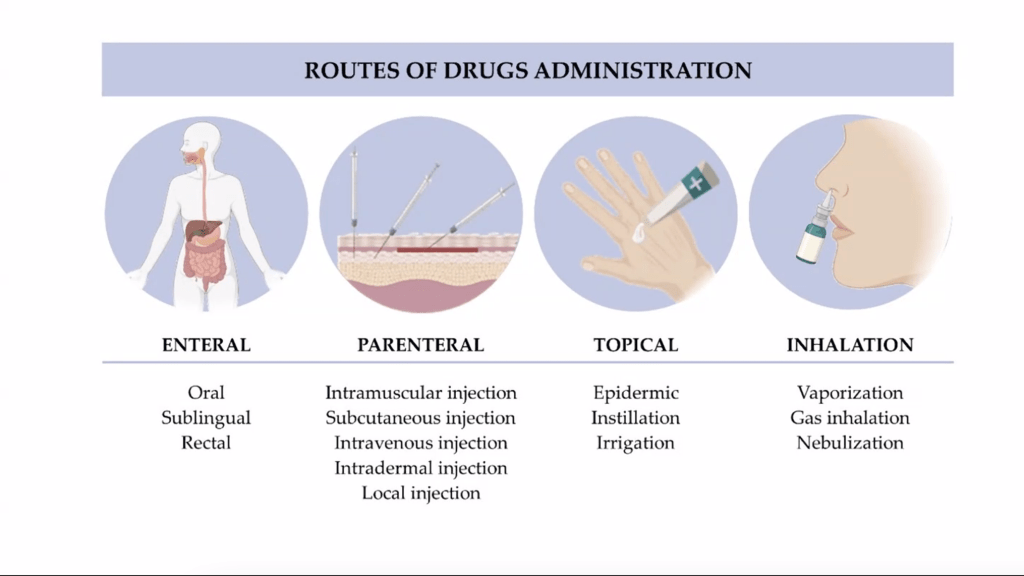
There are, in principle, different routes of drug administration. Very simply put, drugs can be taken through the digestive system, they can be administered parenterally, they can sometimes be administered topically, and—particularly for lung doctors and increasingly in the field of PH—the inhaled route may be considered for many of these drugs.
When we look at the side-effect profiles of many well-established medications, we see some anticipated side effects related to the mechanism of action, as well as some unanticipated off-target effects. These may be related either to the drug’s mechanism or to the route of administration. I would like to dwell a little more on how we might mitigate side effects by considering different administration routes.
The whole story really started in the early 1990s, when the first drug for the treatment of pulmonary arterial hypertension was introduced: continuous intravenous infusion of epoprostenol. By default, this drug had to be administered via a battery-driven pump that was worn outside the body. To bring the drug into the bloodstream, patients needed an indwelling catheter inserted through the skin and ending in one of the central veins or in the right atrium, providing the drug as a continuous infusion.
This treatment can be lifesaving. It improved outcomes for many patients. However, because of the route of administration and the indwelling line, there can be line infections, thrombotic episodes, and catheter dislocations. There are also reports of infusion-pump failure. The costs are enormous, and the drug comes with many systemic side effects because it is administered systemically and therefore acts in all vascular compartments, not only in the desired pulmonary vasculature.
The advancement of treatments and the introduction of distinct drug classes that could be administered orally was therefore already a major step forward. We are talking about endothelin receptor antagonists, phosphodiesterase-5 inhibitors, prostacyclin treatments, as well as soluble guanylate cyclase stimulators, which are at the forefront of oral treatments.
However, as mentioned before, when you administer a drug systemically—in this case orally—the drug distributes systemically and also displays side effects across a multitude of organ systems. The question always remained, particularly for prostacyclin derivatives, whether they might also be administered in different ways.
To overcome specifically the shortcomings of continuous epoprostenol infusion, which requires an indwelling catheter, one step forward was the use of implantable pumps for intravenous prostanoid therapy. These pumps are not battery-driven; they are mechanically driven. The catheter is still placed intravenously, but the entire system is implanted subcutaneously and therefore has no outlet to the outside world. The risk of infection is lower. The chamber can be refilled every two to four weeks, which is quite convenient compared with the daily change of drug cassettes required with epoprostenol therapy.
Naturally, because of the long administration times and the fact that the chamber is connected to body temperature, one has to use a more stable prostacyclin derivative, and therefore this approach has often been used with intravenous treprostinil.
For lung doctors, of course, we have a very special route of access to the region of interest, which is the pulmonary vasculature. The airway space, particularly the alveolar space, is in close proximity to the pulmonary arterial resistance vessels. That is where the disease actually happens and where it progresses—in the small pulmonary arteries of the lung.
If you imagine taking a drug that has already shown efficacy through other administration routes, nebulizing it, inhaling it, and bringing it into the airways in close proximity to the resistance vessels, that was exactly what we first did with inhaled iloprost. In the first patient to inhale iloprost, pulmonary artery pressure could be significantly reduced, cardiac output—the blood flow through the lungs—could be increased, systemic blood pressure could be maintained, and oxygen saturation could even improve.
However, the effects were rather short in duration. So the next step in evolving this concept was to use a longer-acting prostanoid derivative—treprostinil. Treprostinil can be administered not only intravenously or subcutaneously, but also, as we and others showed and later proved in approval studies, through inhalation with a longer duration of efficacy.
Patients on iloprost have to inhale six to nine times daily, while treprostinil in its current formulations has to be inhaled only four times daily, with a considerably shorter inhalation time. Therefore, the development of inhaler technology is key to improving acceptance by our patients.
Meanwhile, with some inhaled prostacyclins, the time needed to apply a dose has been reduced to a few minutes, and with some devices even to just a few breaths. Depending on the molecule and the formulation, the effect can then last for hours. This brings us much closer to the convenience patients know from inhaled therapies in diseases such as asthma or COPD.
Just a few examples from current developments: different drug classes and representatives of those classes can now be used—some of them in investigational trials—in dry-powder formulations. The drug comes as a dry powder, a capsule is placed into a small portable device, the capsule is punctured, and with a deep breath the patient takes in the entire dose. In the case of mosliciguat, an activator of soluble guanylate cyclase that is currently under investigation for patients with pulmonary hypertension and lung fibrosis, this is only once daily, which is quite remarkable.
There are other medications that have just been tested and are still under investigation, such as the tyrosine kinase inhibitor seralutinib. This is also given by dry-powder inhalation. The intention is to reduce systemic side effects by achieving lung deposition while reducing systemic exposure, in contrast to what was seen with oral imatinib.
Coming back to the previously mentioned class of prostacyclins and prostacyclin derivatives, we are now witnessing a very rapid evolution of novel devices as well as new ways of reformulating very well-established drugs.
With one of the latest additions to the therapeutic armamentarium, so-called PRINT technology is used to produce very well-defined nanosized particles that can be delivered through the airways. Unlike other dry powders, where the particle size may be quite inhomogeneous, here the particle size is well defined and lung distribution to the periphery—where the drug is intended to work—is very precise and reproducible.
Ultimately, it is not only a matter of inhalation duration or of the precision with which the inhaled drug reaches the periphery of the lung. It is also a matter of aerosol tolerability. Some dry powders produce cough in our patients, and therefore a further potential evolution could be to encapsulate drugs of interest into so-called liposomes. These are like oily droplets that encapsulate the active drug. In this way, administration can be directed more precisely, the drug can be better tolerated when inhaled into the lung, and, depending on the composition of the capsule, one may even modify the drug release from these micro- or nanocapsules and thereby alter spillover and systemic side effects.
We heard in the previous talks about the importance of monitoring drugs online, if possible in real time, because when we try to target the disease and apply the most suitable drug—or combinations of drugs—to our patients, we also need to understand efficacy. One example is a drug trial performed with an implantable monitor, the CardioMEMS device that Wendy just mentioned, modeling pulmonary pressures and pulmonary resistance in patients. It could even show what happened if the drug was withdrawn, giving us an idea of the durability of the effect.
We can extend this notion by introducing novel technologies. We now have a new device that can help us not only assess classical efficacy parameters for the pulmonary circulation, but in addition gives valuable information about what drugs do to right-heart function. It may help us distinguish between effects on the pulmonary vasculature and effects on the right heart chamber, which will be of great interest for many upcoming drugs.
Allow me to summarize. The classical routes of administration are straightforward: oral, intravenous, subcutaneous, intramuscular, inhaled, and transdermal. The first approved PH drug was intravenous epoprostenol, but it came with drug-related side effects and adverse events related to the route of administration. Oral pulmonary hypertension medications were a major step forward, though they also have drug-specific side effects. The inhaled route is obviously ideal for delivering drugs to the region of interest, thereby reducing systemic exposure.
In the future, combining lung-targeted therapies with online pharmacodynamic monitoring may become key to individualized treatment strategies. Ultimately, the goal is to make these treatments efficacious and, most importantly, well tolerated for our patients.
With that, I would like to send greetings from the German Center for Lung Research, where many researchers and clinicians are working on better drugs and better ways to apply them for the sake of our patients.
Thank you for your attention.
Dr. Andreas Reimann:
Thanks very much, Professor Ghofrani, for this fascinating insight into modern drug-delivery technologies. I was also very happy to see that big picture of the Center for Lung Research. As a German, I am absolutely happy that we have that great network in Germany, and you can be proud of that. Thanks very much.
And now Hall is back with us. He was experiencing some technical issues. Very happy that you are with us, Hall. You are going to share your experience of devices and wearables. The floor is yours.
Hall Skåra:
Thank you so much. Sorry about before. I do not know what happened. I was not allowed to share the screen.
My name is Hall Skåra, and let me say something about my background because I think it might be relevant. I am a patient. I was diagnosed with pulmonary arterial hypertension more than 20 years ago. I also have a computer background. Before I became ill, I worked in a computer company, so that may influence how I view technology today. I also live in Norway, and what I have seen is that here in Norway we perhaps have a little more trust in government and institutions, so we are not so resistant when it comes to sharing data. I am therefore not afraid of digital health and AI.
I have an iPhone and an Apple Watch, so I am definitely an Apple person. The first thing I used these products for was medication reminders. I take medication three times a day. It is easy to remember the morning and the evening doses, but the middle of the day can be a little difficult. Then I get a reminder. Often, when I get the reminder, I do take the medication—but I sometimes forget to click in the app that I have taken it, so the overview is not very impressive. But it does help with medication adherence.
The second thing—especially for those who know Apple products—is that it helps, at least for me, to motivate myself to be more active. You have these rings: a blue ring, which starts to move as soon as you stand up for at least one minute during an hour; a green ring, which indicates exercise, because the watch detects when you are exercising; and a red ring, which shows calories burned.
I have set the limits myself for the amount of exercise and calories burned during the day. The calorie level is the level beyond resting metabolism. I set my goal to 600 because I felt that was reachable. Looking at the last year, I can see I may have been a little optimistic because the average was 395, but I did reach my training goal of 13 minutes every day. In fact, I trained on average 38 minutes over the last year. I am also aware of the need to stand up and not sit for too long, so I stand up in at least 12 separate hours every day on average.
This gives me a good overview of my activity level and perhaps tells me that I am good at exercising, but I could be a little more active outside of those periods when I deliberately exercise.
The Apple Watch will also calculate or estimate your max VO2. Before I got sick, I actually did a proper test just for fun with a friend, and I remember my max VO2 was 51, which is quite good—I was in good shape. When I got sick, it was 16. Of course, you really notice a drop from 51 to 16.
For those who do not know, max VO2 tells you how much oxygen the body is able to use during very intense activity. The Apple Watch now gives me an estimate, and here is the estimate for the last year. Twenty years after my diagnosis, I am far better than I was when I was first diagnosed, but I am of course not at the level I was when I was healthy. What is interesting is to look for the trend.
In my case, I can see a slight downward trend, and that is something I definitely need to talk to my doctor about. When I go for my yearly control, we do not do a six-minute walk test; we do a max VO2 test, so I am able to double-check this at the hospital.
Of course, I also measure my sleep. Here we can see the amount of time spent awake, in REM sleep, in core sleep, and in deep sleep. It is also interesting to see what my pulse is during sleep, because the Apple Watch captures that. I have quite a low pulse. My maximum pulse during sleep was 54, and my minimum was 46. I can also see what my oxygen level was during sleep—in this case between 91 and 100.
This gives me very good data, and it helps me to see trends. If you combine sleep data with breathing frequency, pulse, and oxygen measurements, you may get an indication of whether there could be problems with sleep apnea, which is one of the issues people with pulmonary hypertension might have.
I also use the watch extensively when I exercise. Here is a typical day: in February, I had some exercise around 12 o’clock, so this is when I was out walking, and then I exercised again in the evening. I can see how my oxygen level corresponds to that exercise.
Another thing I find very useful is resting heart rate, because if you see an increase in resting heart rate, that could be an indication that your disease is deteriorating. Here is my resting heart rate over the last year, and, as you can see, it is quite stable between 48 and 51.
It is also amazing what these watches can do. It can even do an ECG. Here is one I did in December, and I could see that it showed a normal sinus rhythm. Then one day in October I felt that my heart was not beating regularly, so I did an ECG myself, exported it as a PDF, and sent it to my doctor. He said, “This looks like extrasystoles, but come to me and we will do a proper ECG and double-check.” I find it very reassuring to be able to do these kinds of things myself.
You can also use fall detection, which is automatic with an Apple Watch. I did fall once while I was out walking my dog in the forest. I had the leash in one hand and the other hand in my pocket, and I fell on my nose, as you can see. I think I was out for a little while because I woke up with the dog licking my face. If it had been more serious and I had been unconscious for longer, the watch would automatically have called emergency services and provided GPS coordinates.
So it is amazing what these watches can do. When I looked into it today, I also saw a lot of things I had not looked at before. For instance, one graph shows how much time I spend outside. I suppose it uses GPS to see when I am outside the house and walking. On average over the last year, I spent a little more than one hour outside every day.
Another curious one is handwashing. It estimates how many times I wash my hands during the day. I do think it underestimates it somewhat when it says that I only wash my hands twice for 10 seconds on average. But for us, living with pulmonary hypertension, it is important to have good hygiene so we do not end up with infections. So perhaps it reminds me that I should wash my hands a little longer and more properly so that it registers more than two times a day.
The next thing Apple is talking about is enabling blood-glucose monitoring in your watch. They have not managed to make this fully work yet, but this will come, and it will be very interesting to be able to follow blood sugar levels and perhaps use this to adjust eating patterns.
I think things like this are very helpful when you talk to your doctor. Instead of simply saying, “I felt worse last month,” you can say, “Last month my max VO2 dropped by 20%, my resting heart rate increased by 10, and my activity level dropped by 25%.” That gives the doctor much more usable information about your situation.
For me, I really embrace this type of technology. It is motivating to me, gives me more insight, helps me detect deterioration in my health earlier, gives me better consultations, and supports more shared decision-making.
I guess some people would say this sounds a little bit like George Orwell’s 1984, and it is ironic because Apple had a very famous ad in 1984 at the Super Bowl about rebelling against that kind of control. They said computers should empower people and not be used to monitor and control them. And that is exactly what I am doing right now with Apple products—but I am choosing to do this myself, and I am choosing who to share the data with.
Q&A session
Dr. Andreas Reimann:
Thanks very much, Hall, for your insights and for sharing that with us. We have a little time left for questions, and I think it is worthwhile to address them.
Let me start with a question directly to you, Hall. Are you able to share the Apple Watch data prior to a meeting with your PH centre?
Hall Skåra:
Yes. For instance, the ECG, as I showed you, can be exported as a PDF and sent to my doctor. All the other data are collected on the phone and on the computer, so I can make copies of them and bring them to my consultation.
Dr. Andreas Reimann:
All right. Now a question, I guess, to Professor Neubeck and Professor Ghofrani, because there were a couple of questions around clinical trials. Are wearables and digital devices already being used as endpoints in clinical trials? Liz, perhaps first, and then Ardeschir.
Prof. Lis Neubeck:
Yes, they are. I think the key point is that they are not really being used as primary endpoints; they are being used as tools to collect data. But if you are considering using a digital wearable device, then it is important to make sure it has the appropriate regulatory approval. That means the manufacturer has had to submit a lot of paperwork and evidence to show that the device is valid. And of course the Apple Watch does have that; others do as well. Whatever you are doing—whether using it in clinical trials or for personal use—you want to make sure it is as accurate as possible.
Dr. Andreas Reimann:
Okay. Thank you very much. Professor Ghofrani, anything to add to that?
Prof. Ardeschir Ghofrani:
Very little to add. With particular attention to pulmonary arterial hypertension trials, the regulatory agencies that ultimately approve drugs still rely very heavily on surrogate outcome measures. In the case of the US Food and Drug Administration (FDA), that is still change in six-minute walk distance, and in the case of the European Medicines Agency (EMA), it is time to clinical worsening or clinical events occurring during a defined observation period.
Having said that, many of the devices and the parameters they measure are currently being investigated in such clinical trials, either as exploratory endpoints and, increasingly, also in ways that may qualify them to become secondary endpoints. We as a scientific community, together with our patients, have to provide the agencies with data they can trust if approvals are ever to be based on these novel types of data. I would personally very much welcome the introduction of novel trial endpoints.
Dr. Andreas Reimann:
Thanks very much. Another question to you, Ardeschir: the new drug-delivery devices and the new routes of administration of pulmonary arterial hypertension drugs—do they have any impact on quality of life? Can we also see that in quality-of-life data?
Prof. Ardeschir Ghofrani:
Yes. I think that is a very important question, because it also highlights what patients’ experiences have been with older drugs and previous treatments they have taken. Of course, in any of the clinical trials we conduct in the field of pulmonary arterial hypertension—as in many other diseases—quality-of-life measures and patient-reported outcomes are also investigated. Some of them specifically address issues related to the route of administration.
Using, again, the example of intravenous treatment with epoprostenol as compared with inhaled drug application, I believe it is quite obvious that patients prefer inhaled administration over the intravenous route.
Dr. Andreas Reimann:
Thanks very much. And my last question to Wendy: Wendy, you were talking about telemedicine. Are you aware of any clinical-trial settings using decentralized or remote approaches where telemedicine was part of the regular visits?
Wendy Gin-Sing:
Yes. We have some trials underway at the moment. One is an observational trial in which patients have an ECG monitor and a CardioMEMS device, and that is basically just following them through the normal course of their clinical care.
But we have also had a trial called Phoenix, where there were different options for intensifying dual therapy: either adding selexipag or switching from a PDE-5 inhibitor to riociguat. Those patients were monitored with CardioMEMS devices. So it was not only about how the patient felt—we were able to see exactly what was happening to their pressures.
We also have studies with imatinib in which one of the primary endpoints is the change in pulmonary artery pressure. So we are certainly using these technologies more, and patients like them because they often do not have to come back for another right-heart catheterization.
Dr. Andreas Reimann:
Okay. Thanks very much. I am aware that we are running a bit over time, but it was really worthwhile because we heard four excellent presentations and had some great questions. Thanks very much for your participation, and thanks also to everyone who will listen to the recording. Please stay tuned for the second webinar in the second quarter of this year.